In the UK, the majority (90%) of hypertension is managed in primary care. Yet, for the 10% who require secondary-care input, there is no specialist register for doctors who manage hypertension. There is a mismatch across the nations with regards to access to secondary care for management of complex hypertension cases. Heterogeneity exists in terms of local specialist services, referral pathways, and specialties overseeing care.
We polled across primary care in the UK to assess accessibility to a local specialist hypertension clinic, the clinical reasons for referral and the specialty referred to. Cardiology was by far and away the leading specialty for referrals. Yet the vast majority of cardiology trainees in the UK are receiving minimal, if any, specialist training in hypertension. A cardiology registrar is likely to spend substantially more days on-call for general medicine than the amount of specialist clinics they can attend in hypertension.
We are facing a major deficit in the specialist management of hypertension if the trainees of today are not ready to provide the required expertise and oversight for the complex cases of tomorrow.
Introduction
Hypertension is a highly prevalent condition affecting nearly a third of UK adults.1 It is estimated that 12.8% of worldwide mortality is caused by hypertension.2 The disease affects all ages, all genders and does not differentiate for deprivation, with incidence grossly unchanged in 20 years and numbers of people potentially undiagnosed ever rising.3 Treating blood pressure costs an estimated £2.1 billion to the National Health Service (NHS) every year.4 Blood pressure control is not optimised in around three million people, putting them at an even greater risk.5
In the UK, >90% of hypertension is managed in primary care. Yet for those who require secondary care input, there is no specialist register for doctors who manage hypertension. Indeed, it is estimated that there are only around 70 experts in hypertension across Great Britain and Ireland. According to 2019 data (National Institute for Health and Care Research – NIHR), approximately 12% of primary care appointments are related to hypertension. At a basic estimate, this equates to at least 36 million appointments in the NHS per year based on hypertension.
There is a mismatch across the nations with regards to access to secondary care for management of complex hypertension cases. Heterogeneity exists in terms of local specialist services, referral pathways, and specialties overseeing care.
In this study, we aimed to identify two measurable factors. First, we set out to clarify which specialty was the most referred to for treating complex hypertension (and the reasons for referral). Second, we set out to quantify and identify who is being trained to manage hypertension in a secondary-care setting, and if this is sufficient for the future needs of the NHS.
Method
We carried out two surveys. The first was in general practice, to assess accessibility to a local specialist hypertension clinic, the clinical reasons for referral, and, most noteworthily, the specialty to which the patient would be referred. We collaborated with the Primary Care Cardiovascular Society (PCCS), who were extremely helpful, to send our survey to their entire network of doctors, pharmacists, practice nurses and all members of the allied health team. This allowed us to have responses from across the four nations, and from a variety of multi-disciplinary team (MDT) members treating hypertension within primary care.
Results were collected online anonymously, with demographics, such as country and respective health board, integrated care board (ICB) or GP federation noted as well. In the online form, we also asked for a 1–10 rating of the local secondary-care hypertension provider, to gauge satisfaction among referrers.
A second survey of hypertension training among cardiology trainees was undertaken. As part of the British Junior Cardiologists Association’s (BJCA) annual survey, trainees were asked whether they had had “any training in hypertension at a specialist hypertension clinic, or from a consultant specialist in hypertension”. This survey was distributed through online mailing lists and via the BJCA network of regional representatives to their approximately 1,000 members, representing the majority of cardiology trainees in the UK. Of these, 419 trainees responded to this question on hypertension training. These results were collated by the BJCA and compared, with regional variances noted.
Results
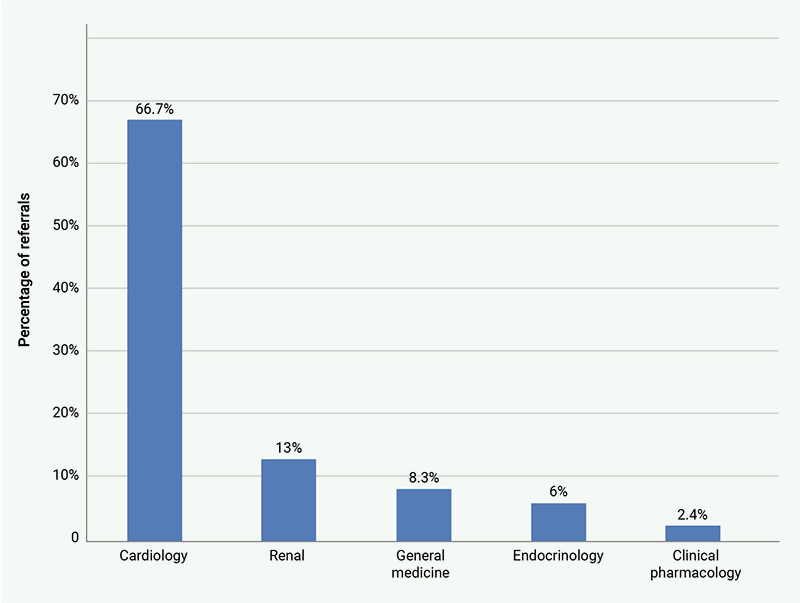
The separate survey results have shown two clear and distinct outcomes. First, that cardiology is by far the most frequently referred to specialty for hypertension where no local specialist clinic is available (figure 1). Of 130 respondents, 66.7% of referrals were to cardiology, followed by renal medicine (13%), general medicine (8.3%) then endocrinology (6%). Of note, only 2.4% of referrals were directed to clinical pharmacology.
Of the further data from primary care, multiple answers were allowed when capturing clinical reason for referral: 92.2% of respondents stated resistant hypertension as one of their causes, followed by hypertension in those aged 18–39 years at 59.7% of referrals and intolerable side effects of antihypertensive medication as third most frequent at 34.1% of referrals. Of respondents, 14% stated their referral was at least in part for ambulatory blood pressure monitoring (ABPM), highlighting the ongoing limitation of this testing in the NHS. Assessing satisfaction of their local secondary care hypertension service out of 10, the mean rating was only 6.25.
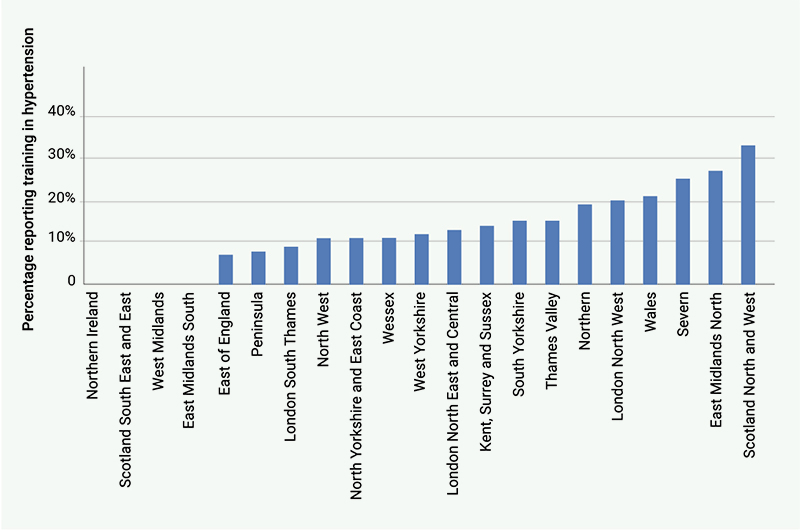
The second clear result was the lack of training cardiology trainees are receiving in hypertension. Of the BJCA trainees, 87.6% of trainees stated that they had never had any specialist hypertension training (figure 2). The geographical variance was notable, and indeed in multiple regions, this number rose to 100% of trainees reporting no training of any kind in hypertension.
Discussion
Meeting service requirements is a challenge across the NHS. Waiting times are a national issue, which the government has pledged to address. Currently, the British Heart Foundation (BHF) reports that at least 40% of patients exceed the standard 18-week wait for a first outpatient appointment in cardiology. This figure could skyrocket for hypertension referrals based on our data.
The data from primary care is clear – the majority of referrals in the UK for hypertension go to cardiology. And yet, the trainees in cardiology receive little to no training in hypertension in the secondary-care setting. Cardiology registrars are examined in hypertension as part of the European Examination in Core Cardiology, yet rarely, if ever, have opportunities to put this into practice as trainees, yet are expected to be experts as soon as they become a consultant.
So, who should offer training in the management of high blood pressure? And to whom? A quick glance at the 2026 programmes for the annual scientific meetings (ASMs) of the Society of Endocrinology and UK Kidney Week,6,7 the leading annual events for endocrinologists and renal physicians in the UK, shows no sessions about essential hypertension. The British Cardiovascular Society’s (BCS) ASM always has at least one full session devoted to hypertension, and is well attended, but can do more, and the BCS needs to strengthen its learning courses in high blood pressure for trainees in cardiology. The British and Irish Hypertension Society (BIHS) sets many UK standards for hypertension, but does little teaching for GPs, and none for cardiologists in training.
So, we suggest that the BIHS and BCS work with the Joint Royal Colleges of Physicians Training Board (JRCPTB) to include hypertension as a defined core part of specialist training in cardiology. After local soundings, we suggest attendance by cardiology specialist trainees at five to six hypertension clinics within their training district, over the four years of specialist training. This is hardly a large percentage of their training time.
And for GPs? In our view the BIHS must work far more closely with GP bodies like the PCCS to develop and maintain training programmes in hypertension. BCS could do this too.
Hypertension is one of the most prevalent conditions in the UK. Cardiology is the usual specialty for referrals, and we must prepare our trainees accordingly.
Key messages
- The majority of referrals in the UK for hypertension go to cardiology
- Trainees in cardiology receive little to no training in hypertension in the secondary-care setting
- We are facing a major deficit in the specialist management of hypertension if the trainees of today are not ready to provide the required expertise and oversight for the complex cases of tomorrow
Conflicts of interest
None declared.
Funding
None.
Acknowledgement
The recently deceased, Professor Adrian Brady, co-authored this article and we would like to dedicate it to him in his memory. He will be greatly missed.
Editors’ note
*Professor Brady did not give final approval of the article but James Brady, his next of kin, did so in his stead.
Please also see the editorial at https://doi.org/10.5837/bjc.2026.029.
References
1. British Heart Foundation. UK Cardiovascular Disease Factsheet. London: BHF, September 2025. Available from: https://www.bhf.org.uk/what-we-do/our-research/heart-statistics/heart-statistics-publications [accessed September 2025].
2. World Health Organization. Global status report on noncommunicable diseases 2010. Geneva: WHO Press, 2010. Available from: https://iris.who.int/handle/10665/44579
3. NHS England. Health Survey for England 2021, part 2. Adults’ health: Hypertension. May 2023. Available at: https://digital.nhs.uk/data-and-information/publications/statistical/health-survey-for-england/2021-part-2/adult-health-hypertension
4. UK Health Service Agency. Health matters: combating high blood pressure. January 2017. Available at: https://ukhsa.blog.gov.uk/2017/01/24/health-matters-combating-high-blood-pressure/
5. British Heart Foundation. Personalised treatment could be key to tackling uncontrolled high blood pressure. September 2024. Available at: https://www.bhf.org.uk/what-we-do/news-from-the-bhf/news-archive/2024/september/personalised-treatment-could-be-key-to-tackling-uncontrolled-high-blood-pressure
6. Society for Endocrinology. Scientific programme. 2026. Available at: https://www.endocrinology.org/events/sfe-bes-conference/sfe-bes-2026/scientific-programme/
7. UK Kidney Week. Programme at a glance. 2026. Available at: https://www.ukkw.org/3d-flip-book/2026-programme/
