Introduction
Heart valve disease is as common as heart failure. The population prevalence is 2.5% rising to over 10% in people aged more than 75.1
It has received disproportionately little exposure in terms of research, national treatment strategies and public awareness. This is beginning to change, partly with a rise in prevalence as our population ages and partly as a result of technological advances including transcatheter procedures. In this module we will describe the causes and frequency of valve disease. We will also discuss variations in the delivery of care.
Causes of valve disease
Temporal and geographical trends
Rheumatic fever is the most common cause of valve disease in the young2 but predominates in industrially underdeveloped regions. These include Africa, India, the Middle East, South America, parts of China and Russia, and the aboriginal populations within Australia and New Zealand.

For further information on rheumatic fever and its consequences, with the development of rheumatic heart disease, see this World Heart Federation video outlining the public health challenges of this condition
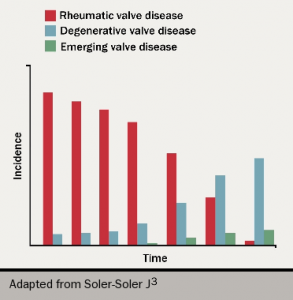
In industrially developed countries, the incidence of rheumatic disease declined after the second half of the 20th century (see figure 1). With increased longevity, valve conditions characteristic of old-age now predominate. The most common are calcific aortic stenosis and functional mitral regurgitation.
There has also been a rise3 in new diseases induced by drugs or therapeutic irradiation, an increase in endocarditis related to intravenous drug use, device implantation and haemodialysis and a rise in the number of operations as a result of failing replacement heart valves.
Drugs
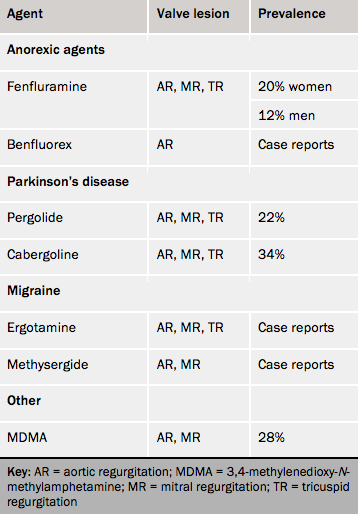
The valve lesions caused by drugs resemble those from carcinoid tumours. These arise from neural crest gastrointestinal enterochromaffin cells in 1 in 75,000 people.4 The carcinoid syndrome develops in about one half as a result of hepatic spread and carcinoid heart disease develops in 40% of these. The cardiac lesions are caused by the paraneoplastic effects of vasoactive substances, notably 5-hydroxytryptophan (5HT). The drugs known to cause valve disease (see table 1) are either themselves or have metabolites that are agonists at 5HT2B receptors.
Drug-induced lesions are similar to those found in carcinoid disease.
Interaction with the 5-HT2B receptor stimulates cardiac fibroblast proliferation leading to fibrous plaques with a ‘pearly white’ appearance on valves and chordae.
The earliest sign of valve involvement is an increase in the tenting height of the mitral valve, which is the distance between the point of apposition and the plane of the annulus.
Pergolide and cabergoline cause valve disease when used in the relatively large doses necessary for Parkinson’s disease. With the small doses used for microprolactinoma, valvopathy appears to be rare, but can occur after relatively large doses used for periods in excess of 10 years.
