Refractory angina (RA) is characterised by persistent anginal symptoms despite optimal medical therapy and revascularisation. Enhanced external counterpulsation (EECP) is a technique that has shown promise in the treatment of this condition but is poorly utilised in the UK. The aim of this study is to assess the effect of EECP on anginal symptoms in patients with RA from a UK centre.
This retrospective study assessed the effectiveness of EECP at improving exercise capacity, anginal symptom burden and anginal episode frequency using pre- and post-treatment six-minute walk test (6MWT) results, Canadian Cardiovascular Society (CCS) scores and symptom questionnaires, respectively.
Fifty patients with a median age of 67 years (interquartile range [IQR] 14) underwent EECP between 2004 and 2015. The majority had undergone prior revascularisation (84%; 42/50) via percutaneous coronary intervention (PCI) and/or coronary artery bypass grafting (CABG). Significant improvements were noted in 6MWT result (282 vs. 357 m; p<0.01), CCS score (3.2 vs. 2.0; p<0.01) and weekly anginal episode frequency (20 vs. 4; p<0.01). No adverse outcomes related to EECP were noted.
Our study demonstrates use of EECP to be associated with significant improvements in exercise capacity and anginal symptom burden.
Introduction
Angina pectoris is the most common symptomatic manifestation of ischaemic heart disease (IHD), and is usually caused by an imbalance between myocardial oxygen supply and demand. Standard therapy for angina pectoris includes pharmacological agents, such as rate-limiting drugs and vasodilators. When symptoms are not satisfactorily controlled by pharmacotherapy alone, revascularisation via either percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG) has been demonstrated to be of benefit in certain circumstances.1,2
While the majority of patients with angina pectoris can be managed successfully using a strategy of pharmacotherapy and revascularisation, there remains a subset that suffer with persistent symptoms despite these measures. The term ‘refractory angina’ (RA) is used to denote this chronic and debilitating condition and, while definitive epidemiological data pertaining to the prevalence of RA is scarce, there is a general recognition that it is a growing problem, and one that results in a significant public health burden.3 Management of this condition is often challenging, and so research into alternative treatment modalities has generated interest in recent years. Examples of techniques that have been investigated include trans-myocardial laser revascularisation,4 spinal cord stimulation,5 and coronary sinus reducer implantation.6 While these treatments have demonstrated varying levels of success, the 2013 European Society of Cardiology (ESC) guidelines for the management of stable coronary artery disease highlighted enhanced external counterpulsation (EECP) as the non-pharmacological treatment with the best evidence base for the treatment of RA.7
EECP is a technique that works on the principle of using aortic counterpulsation in order to augment diastolic blood flow. Pressure cuffs are wrapped around the lower limbs of patients and inflated at the onset of diastole, thereby increasing diastolic blood pressure. This has the effect of improving coronary perfusion pressure during diastole. The rapid deflation of the cuffs at the onset of systole also serves to reduce vascular resistance, causing a reduction in cardiac workload.8 The combined effect is analogous to that of an intra-aortic balloon pump (IABP), albeit in a non-invasive fashion.
Clinical trials utilising EECP in patients with RA have been encouraging. The landmark MUST-EECP study (Multicenter Study of Enhanced External Counterpulsation) was a randomised-controlled trial (RCT) that demonstrated EECP to be associated with a significant improvement in time to ST-segment depression on stress testing, as well as a significant decrease in angina frequency among patients with RA.9 Subsequently, a number of studies have corroborated these findings, and, indeed, meta-analyses have demonstrated EECP to be associated with improvements in anginal symptom burden,10,11 and myocardial perfusion.12 Based upon this body of evidence, EECP has become established as a treatment for RA in North America, China, Russia, India and the Middle East. In contrast, utilisation of the technique in the UK has been poor,13 and, indeed, current guidelines for the management of stable angina from the National Institute for Health and Care Excellence (NICE) do not advocate its use.14
The aim of this study is to assess the effect of EECP on functional exercise capacity and anginal symptom burden in a real-world population of patients with RA, based upon data from one of the few UK centres with experience in the technique.
Method
This study was carried out as a single-centre, retrospective analysis of patients who underwent EECP. The decision to initiate EECP was made by the cardiology team following a multi-disciplinary review of patients’ symptoms, medication regimens, results from functional imaging, and revascularisation options. Patients eligible for EECP were those with disabling refractory angina (Canadian Cardiovascular Society [CCS] score ≥3) despite at least three anti-anginal agents, evidence of inducible ischaemia on myocardial perfusion scanning and no options for revascularisation based upon a coronary angiogram from within the preceding 12 months (figure 1).

EECP therapy is delivered over the course of seven weeks, with 35 hour-long sessions. Three sets of cuffs are wrapped around the patients’ calves, lower thighs and upper thighs, and patients are monitored by means of electrocardiography (ECG) and finger plethysmography. Timing of inflation is determined primarily by the ECG tracing, with cuff inflation occurring sequentially at the onset of diastole, and deflation at the onset of systole. The plethysmographic waveforms are used in order to monitor systolic and diastolic waveforms, allowing further optimisation of inflation timing.
Two weeks prior to EECP, all patients underwent an assessment of functional exercise capacity by means of a six-minute walk test (6MWT). Anginal symptom burden was assessed by use of the CCS scoring system and quantification of anginal episodes per week, both of which were patient-reported. These measures were subsequently repeated two weeks following the completion of the EECP regimen, and the results documented in the patients’ records. Data for this study were collected retrospectively from these records, allowing for a comparison between pre- and post-treatment functional status and symptoms. Further information on patients’ demographics, coronary anatomy, medication regimen, history of revascularisation and functional imaging results was also collected. No changes to anti-anginal medications were made during the EECP treatment period.

For the purposes of this study, each patient who had undergone EECP between 2004 and 2015 was assigned a number, and 50 were selected for analysis based on the results of a random number generator. Data collation and statistical analyses were performed using Microsoft Excel for Mac 2011. Continuous variables are presented as means with standard deviations (SD). Parametric data were compared using two-tailed, paired student’s t-test, while the Wilcoxon Signed-Rank test was used for non-parametric data. P values of less than 0.05 were deemed to be of statistical significance.
Results
The study included 50 patients (table 1) who underwent EECP between 2004 and 2015, all of whom completed the 35-hour course. The median age at the time of first EECP therapy was 67 years (interquartile range [IQR] 14), and all but one of the patients was male (98%; 49/50). The majority had a history of prior myocardial infarction (66%; 33/50) and revascularisation (84%; 42/50). Over half of the cohort had undergone prior CABG (68%; 34/50) and all but three demonstrated flow-limiting disease on their most recent coronary angiogram (94%; 47/50). Interestingly, one patient had no evidence of epicardial coronary artery disease despite demonstrable ischaemia on myocardial perfusion scanning, suggestive of cardiac syndrome X.

The majority of patients in the cohort had a diagnosis of hypertension (66%; 33/50), while a sizeable proportion also suffered with diabetes mellitus (34%; 17/50) and hypercholesterolaemia (48%; 24/50). All of the patients were prescribed at least three anti-anginal agents (including one rate-limiting drug), and the majority were prescribed a statin (94%; 47/50) and either an angiotensin-converting enzyme (ACE) inhibitor or angiotensin receptor 2 blocker (82%; 41/50). Other than the single patient with normal coronary arteries, all were prescribed at least one antiplatelet agent (98%; 49/50).
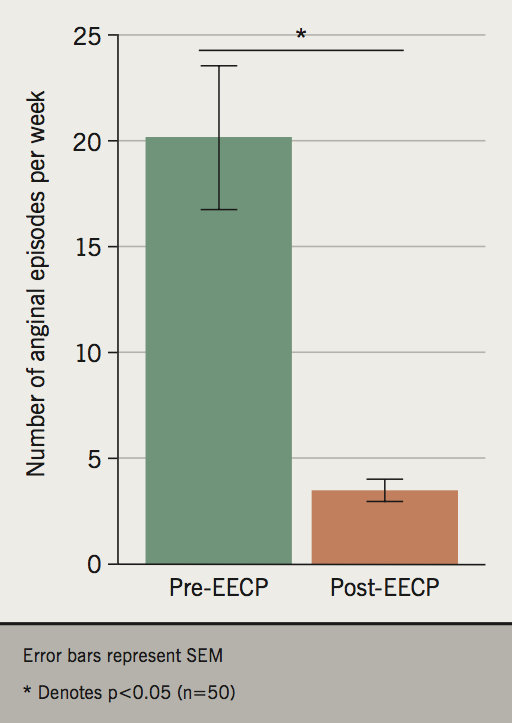
Analysis of pre- and post-EECP 6MWT results demonstrates a significant improvement in functional exercise capacity (282 vs. 357 m; p<0.01) (figure 2). Furthermore, significant improvements were also noted in anginal symptom burden (CCS score 3.2 vs. 2.0; p<0.01) (figure 3) and frequency of anginal episodes (20.1 vs. 3.5 per week; p<0.01) (figure 4). No adverse outcomes related to EECP were noted during the study period.

Discussion
The present study evaluated the effect of EECP on functional exercise capacity and anginal symptom burden among patients with RA, inducible ischaemia and no remaining coronary revascularisation options. We have demonstrated that a full course of EECP is associated with significant improvements in 6MWT results, as well as CCS score and anginal episode frequency. These findings are consistent with previously published data.9,10,15
Analysis of the characteristics of the patients included in the present study highlight that the majority are male and have undergone prior coronary revascularisation. These findings are broadly consistent with those from the landmark MUST-EECP trial.9 Interestingly, the most common pre-EECP CCS score among patients included in the aforementioned RCT was 2. In contrast, every patient included in the present study had a CCS score of at least 3, indicating that our study assessed a more symptomatic cohort. This suggests that the benefit of EECP demonstrated in MUST-EECP is maintained when the technique is applied to patients with a greater symptomatic burden.
The finding of symptomatic benefit with EECP in a real-world RA population is encouraging, especially in light of the challenging nature of the condition being treated. Multiple treatment modalities are often utilised, including pharmacotherapy, revascularisation and psychotherapy,16 and, yet, patients with RA often remain symptomatic despite these interventions. Due to the chronic nature of RA, potential new therapeutic options need to demonstrate financial viability, as well as clinical efficacy. In addition to the multitude of studies demonstrating the symptomatic benefit of EECP, the technique has also been shown to be effective in reducing hospital costs in RA patients.17 Data collected from phase II of the International EECP Patient Registry (IEPR-II) demonstrated a significant reduction in the rate of hospitalisation following EECP, resulting in an annual cost saving of $17,074 per patient.
While there now exists a significant body of evidence in support of EECP, there remains uncertainty regarding the mechanism by which it delivers benefit. A number of theories have been postulated, most of which pertain to two closely intertwined concepts; augmented angiogenesis and improved endothelial function.8 The raised diastolic pressure resultant from EECP has been demonstrated to be associated with increased shear stress, which can stimulate pro-angiogenic factors such as nitric oxide (NO) and vascular endothelial growth factor (VEGF).18,19 The subsequent increase in angiogenesis is hypothesised to be responsible for increased collateral formation within the coronary circulation. EECP has also been shown to improve indices of endothelial dysfunction, with studies demonstrating EECP to be associated with significant improvements in reactive hyperaemia-peripheral arterial tonometry,20 and flow-mediated vasodilatation.21 Furthermore, following EECP, patients with coronary artery disease have been noted to have a significant increase in plasma concentration of the potent vasodilator NO (estimated via measurement of the stable metabolites nitrate and nitrite), and a concomitant decrease in the plasma concentration of the vasoconstricting molecule endothelin-1.22 Finally, EECP has been shown to be associated with a reduction in pro-inflammatory cytokines such as tumour necrosis factor-α (TNFα) and vascular cell adhesion molecule-1 (VCAM-1), which are known to have deleterious effects on endothelial function. Taken together, these mechanisms provide a potential explanation for observed improvements in perfusion scan ischaemia associated with EECP,23 and, thus, may also explain the consistent symptomatic improvements seen among patients in clinical trials, as well as real-world cohorts.
The present study has certain limitations that must be borne in mind when appraising the results. It is a single-centre study with a relatively small sample size. Furthermore, the fact that all of the data were obtained retrospectively meant that there was a dependence on previously acquired data, which may have been of variable quality and validity. Finally, the lack of a control group precludes an assessment of the extent to which the placebo effect contributed to the observed results; the recently published ORBITA (Objective Randomised Blinded Investigation With Optimal Medical Therapy of Angioplasty in Stable Angina) study highlights the importance of the placebo effect when assessing procedural treatments for angina pectoris, as PCI was shown to confer no improvement in symptoms when compared with a sham procedure.24 Nevertheless, while keeping these caveats in mind, the fact that our findings convincingly corroborate those from previously published studies8-12,15 provides validity to our observations.
Conclusion
RA is a chronic disease that is associated with debilitating morbidity and compromised quality of life. In recent years, there has been interest in alternative treatments for patients who remain symptomatic despite being established on optimal medical therapy and in whom revascularisation options have been exhausted. EECP is a non-invasive treatment with encouraging evidence in the RA population. In spite of this, it is relatively under-utilised in the UK. The purpose of the present study was to provide real-world data from a UK centre in order to assess the effect of EECP on functional exercise tolerance and anginal symptom burden. Our data demonstrate that a full course of EECP is associated with significant improvements in 6MWT results and CCS score.
Key messages
- Enhanced external counterpulsation (EECP) is a non-invasive technique that has shown promise in the treatment of refractory angina (RA), based upon results of prior clinical trials and its use in other countries. Nevertheless, it remains under-utilised in the UK
- This study provides real-world data on the effectiveness of EECP in the treatment of RA from one of the few UK centres with experience in the technique. It demonstrates use of EECP to be associated with significant improvements in anginal symptoms and exercise tolerance
- We hope that the results from this study encourage UK cardiologists to reconsider EECP as an effective and viable treatment for RA
Acknowledgement
NA and HJ have contributed equally to this manuscript and have joint first authorship.
Conflict of interest
None declared.
References
1. De Bruyne B, Pijls NH, Kalesan B et al. Fractional flow reserve-guided PCI versus medical therapy in stable coronary disease. N Engl J Med 2012;367:991–1001. https://doi.org/10.1056/NEJMoa1205361
2. Davies RF, Goldberg AD, Forman S et al. Asymptomatic Cardiac Ischemia Pilot (ACIP) study two-year follow-up: outcomes of patients randomized to initial strategies of medical therapy versus revascularization. Circulation 1997;95:2037–43. https://doi.org/10.1161/01.CIR.95.8.2037
3. Banai S, Ben Muvhar S, Parikh KH et al. Coronary sinus reducer stent for the treatment of chronic refractory angina pectoris. J Am Coll Cardiol 2007;49:1783–9. https://doi.org/10.1016/j.jacc.2007.01.061
4. Horvath KA, Cohn LH, Cooley DA et al. Transmyocardial laser revascularization: results of a multicenter trial with transmyocardial laser revascularization used as a sole therapy for end-stage coronary disease. J Thorac Cardiovasc Surg 1997;113:645–53. https://doi.org/10.1016/S0022-5223(97)70221-6
5. Hautvast RWM, Blanksma PK, DeJongste MJL et al.; for the Working Group on Neurocardiology. Efficacy of spinal cord stimulation as adjuvant therapy for intractable angina pectoris: a prospective, randomized clinical study. J Am Coll Cardiol 1994;23:1592–7. https://doi.org/10.1016/0735-1097(94)90661-0
6. Verheye S, Jolicoeur EM, Behan MW et al. Efficacy of a device to narrow the coronary sinus in refractory angina. N Engl J Med 2015;372:519–27. https://doi.org/10.1056/NEJMoa1402556
7. European Society of Cardiology guidelines for the management of stable coronary artery disease: The Task Force on the management of stable coronary artery disease of the European Society of Cardiology (ESC). Eur Heart J 2013;34:2949–3003. https://doi.org/10.1093/eurheartj/eht296
8. Arora RR, Shah AG. The role of enhanced external counterpulsation in the treatment of angina and heart failure. Can J Cardiol 2007;23:779–81. https://doi.org/10.1016/S0828-282X(07)70826-7
9. Arora RR, Chou TM, Jain D et al. The multicenter study of enhanced external counterpulsation (MUST-EECP): effect of EECP on exercise-induced myocardial ischemia and anginal episodes. J Am Coll Cardiol 1999;33:1833–40. https://doi.org/10.1016/S0735-1097(99)00140-0
10. Zhang C, Liu X, Wang X et al. Efficacy of enhanced external counterpulsation in patients with chronic refractory angina on Canadian Cardiovascular Society (CCS) angina class. Medicine (Baltimore) 2015;94:2002. https://doi.org/10.1097/MD.0000000000002002
11. Barsness G, Feldman AM, Holmes DR Jr et al. The International EECP Patient Registry (IEPR): design, methods, baseline characteristics, and acute results. Clin Cardiol 2001;24:435–42. https://doi.org/10.1002/clc.4960240604
12. Qin X, Deng Y, Wu D et al. Does enhanced external counterpulsation (EECP) significantly affect myocardial perfusion? A systematic review & meta-analysis. PLoS One 2016;11:e0151822. https://doi.org/10.1371/journal.pone.0151822
13. Roberts R. Correspondence: is it time for a re-assessment of EECP in the UK? Br J Cardiol 2014;21:51. Available from: https://bjcardio.co.uk/2014/06/correspondence-is-it-time-for-a-re-assessment-of-eecp-in-the-uk/
14. National Institute for Health and Care Excellence. Stable angina: management. CG126. London: NICE, August 2016. Available from: https://www.nice.org.uk/guidance/cg126
15. Bozorgi A, Mehrabi Nasab E, Sardari A et al. Effect of enhanced external counterpulsation (EECP) on exercise time duration and functional capacity in patients with refractory angina pectoris. J Tehran Heart Cent 2014;9:33-7. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4277789/
16. Moore RKG, Groves DG, Bridson JD et al. A brief cognitive-behavioural intervention reduces hospital admissions in refractory angina patients. J Pain Symptom Manage 2007;33:310–16. https://doi.org/10.1016/j.jpainsymman.2006.10.009
17. Lawson WE, Hui JC, Kennard ED et al. Enhanced external counterpulsation is cost-effective in reducing hospital costs in refractory angina patients. Clin Cardiol 2015;38:344–9. https://doi.org/10.1002/clc.22395
18. Masuda D, Nohara R, Hirai T et al. Enhanced external counterpulsation improved myocardial perfusion and coronary flow reserve in patients with chronic stable angina; evaluation by 13N-ammonia positron emission tomography. Eur Heart J 2001;22:1451–8. https://doi.org/10.1053/euhj.2000.2545
19. Masuda D, Nohara K, Kataoka K et al. Enhanced external counterpulsation promotes angiogenesis factors in patients with chronic stable angina. Circulation 2001;104(17 suppl II):II445.
20. Bonetti PO, Barsness GW, Keelan PC et al. Enhanced external counterpulsation improves endothelial function in patients with symptomatic coronary artery disease. J Am Coll Cardiol 2003;41:1761–8. https://doi.org/10.1016/S0735-1097(03)00329-2
21. Braith RW, Conti CR, Nichols WW et al. Enhanced external counterpulsation improves peripheral artery flow mediated dilatation in patients with chronic angina: a randomized sham-controlled study. Circulation 2010;122:1612–20. https://doi.org/10.1161/CIRCULATIONAHA.109.923482
22. Davies PF. Flow-mediated endothelial mechanotransduction. Physiol Rev 1995;75:519–60. https://doi.org/10.1152/physrev.1995.75.3.519
23. Eslamian F, Aslanabadi N, Mahmoudian B et al. Therapeutic effects of enhanced external counterpulsation on clinical symptoms, echocardiographic measurements, perfusion scan parameters and exercise tolerance test in coronary artery disease patients with refractory angina. Int J Med Sci Public Health 2013;2:179–87. https://doi.org/10.5455/ijmsph.2013.2.179-187
24. Al-Lamee R, Thompson D, Dehbi HM et al. Percutaneous coronary intervention in stable angina (ORBITA): a double-blind randomised controlled trial. Lancet 2018;391:31–40. https://doi.org/10.1016/S0140-6736(17)32714-9
