Conduction system pacing (CSP) ― encompassing His-bundle pacing (HBP) and left bundle-branch area pacing (LBBAP) ― delivers more physiological ventricular pacing compared with traditional right ventricular (RV) pacing. It is gaining traction beyond tertiary centres, however, evidence from district general hospitals (DGHs) remains limited. We aimed to evaluate the feasibility, electrical performance, and early clinical outcomes of CSP implemented in a UK DGH.
We performed a retrospective single-centre study of consecutive patients who underwent successful CSP at Chesterfield Royal Hospital. HBP implants (n=20) were performed between June 2019 and August 2022; LBBAP implants (n=71) between January 2023 and May 2025. Baseline demographics, procedural metrics, pacing parameters, complications, heart-failure (HF) readmissions, and echocardiographic data to 12 months were obtained from electronic records.
Ninety-one patients (mean age 76 ± 10 years; 69% male) received CSP, most commonly for left ventricular systolic dysfunction (LVSD) (40%) or anticipated high right-ventricular pacing burden (42%). LBBAP demonstrated lower implant thresholds than HBP (0.92 ± 0.44 V vs. 1.50 ± 0.77 V) and remained stable to 12 months (0.68 ± 0.25 V). HBP thresholds rose to 2.11 ± 1.49 V at 12 months. Screening time was shorter with LBBAP (9.6 ± 5.9 min) than HBP (14.4 ± 6.8 min, p<0.01). No infections or septal haematomas occurred. Lead revision was required in two HBP recipients and none with LBBAP (hazard ratio 17.14, p=0.067). Nine patients (9.9%) were readmitted with HF, occurring between 56 and 1,500 days post-implant.
In conclusion, CSP can be implemented safely and effectively in a DGH setting. LBBAP offers superior electrical stability, shorter procedure time, and less lead revisions, supporting its preferential adoption as the default pacing strategy for CSP.
Introduction
The development of conduction system pacing (CSP) marks a significant advancement in cardiac pacing, offering a more physiological approach by directly stimulating the heart’s native conduction pathways (figure 1).1 In contrast, conventional right ventricular (RV) pacing can result in electrical dyssynchrony, and has been linked to adverse cardiac remodelling and pacing-induced cardiomyopathy over time.2
The two main modalities of CSP – His-bundle pacing (HBP) and left bundle-branch area pacing (LBBAP) – have shown promising results in managing both bradyarrhythmias and heart failure.1,3 While HBP most closely mimics natural conduction by capturing the His–Purkinje system directly, it is technically more challenging, and may be limited by high pacing thresholds and issues with lead stability.1 LBBAP, on the other hand, has seen rapid clinical adoption due to its wider anatomical target, relative procedural simplicity, and reliable electrical parameters.4
Most of the published evidence on CSP has come from high-volume tertiary electrophysiology centres, however, its uptake in district general hospitals (DGHs) is now growing steadily.5,6 This trend reflects increasing confidence in CSP’s safety, reproducibility, and clinical benefit across a broader range of healthcare settings.
In this article, we present our experience with CSP – including HBP and LBBAP – at Chesterfield Royal Hospital, a DGH in the UK. We outline the practical and technical aspects of introducing these techniques, and compare clinical, electrical, and procedural outcomes between the two approaches.
Method
This was a retrospective, single-centre observational study conducted at Chesterfield Royal Hospital. The study reviewed consecutive patients who underwent successful implantation of either a HBP or LBBAP lead between January 2023 and May 2025 for LBBAP (71 procedures) and June 2019 to August 2022 for HBP (20 procedures). Both de novo implants and system upgrades were included. Consecutive patients who underwent successful implantation of either a HBP or LBBAP lead during the respective study periods were included. Successful implantation was defined as stable lead position with confirmed electrical capture of the conduction system. Data on patient demographics, presenting symptoms, pacing indication, procedural characteristics, and follow-up outcomes were obtained from clinical records and the device follow-up clinic.
All CSP procedures were performed under continuous 12-lead electrocardiogram (ECG) monitoring, with the pacing system analyser (PSA) connected to an external catheter laboratory monitor. Devices and delivery systems from two manufacturers, Medtronic and Biotronik, were used at our centre. For Medtronic cases, the C315 pre-shaped catheter was employed for LBBAP procedures, while the C304-HIS deflectable catheter was used in earlier HBP cases. The Medtronic 3830 lumenless lead with a fixed helix was utilised for all Medtronic CSP procedures. For Biotronik cases, Selectra 3D pre-shaped catheters and the Solia S stylet-driven lead were used.
Fluoroscopic guidance was undertaken in both left anterior oblique (LAO) and right anterior oblique (RAO) projections to identify the optimal target site for penetration of the interventricular septum, supplemented by electrical mapping to confirm appropriate positioning. Lead penetration was performed under continuous fluoroscopy in the LAO projection. Contrast injection to delineate septal anatomy and confirm lead depth was used selectively, depending on operator preference and renal function.
Lead advancement into the interventricular septum was guided by pace-mapping using continuous 12-lead ECG monitoring and analysis of unipolar paced QRS morphology during lead rotations. Impedance and injury current were closely monitored throughout this process. Continuous electrical monitoring during lead rotation was only possible for stylet-driven systems, as the Medtronic 5944RL rotatable connector for the 3830 lumenless lead was not yet available during the study period.
Procedural metrics, including screening time, pacing thresholds, R-wave amplitudes, and impedance were recorded at the time of implantation. Successful left bundle-branch area capture was defined by the presence of a terminal R-wave in V1, a left ventricular activation time (LVAT) in V6 of <75 ms (or <85 ms in challenging cases such as intrinsic left bundle-branch block), and a V6–V1 interpeak interval >30 ms. Pacing measurements were repeated at day 1, one month, six months, and 12 months, where available.
Clinical follow-up included echocardiographic assessment of left ventricular ejection fraction (LVEF), comparison with pre-implant echocardiogram, and hospitalisations for heart failure (HF). Complications, such as lead revision, device infection, haemorrhage and septal haematoma, were also recorded. Long-term outcomes were collected up to the date of last follow-up or death.
Results
A total of 91 patients underwent successful CSP. The mean age in the LBBAP cohort was 75 ± 11 years, compared with 77 ± 9 years in the HBP group. In both cohorts, the majority of patients were male (LBBAP 70%, HBP 65%).
Most implants were de novo (79%), with 15 cases (21%) involving system upgrades, including one patient who required an upgrade from HBP to LBBAP. The indications for pacing were atrioventricular (AV) block (37%), sinus node disease (15.3%), and atrial fibrillation (47.5%). CSP indications included left ventricular systolic dysfunction (LVSD) (40%), failed cardiac resynchronisation therapy (CRT) (3.3%), anticipated high RV-pacing burden with preserved left ventricular (LV) function (27.8%), and anticipated high RV-pacing burden with LVSD (14.5%). In 13 patients (14.3%) CSP was undertaken at the consultant’s discretion, including patients planned for AV nodal ablation and younger patients with a conventional pacing indication who may develop higher pacing requirements in the future.
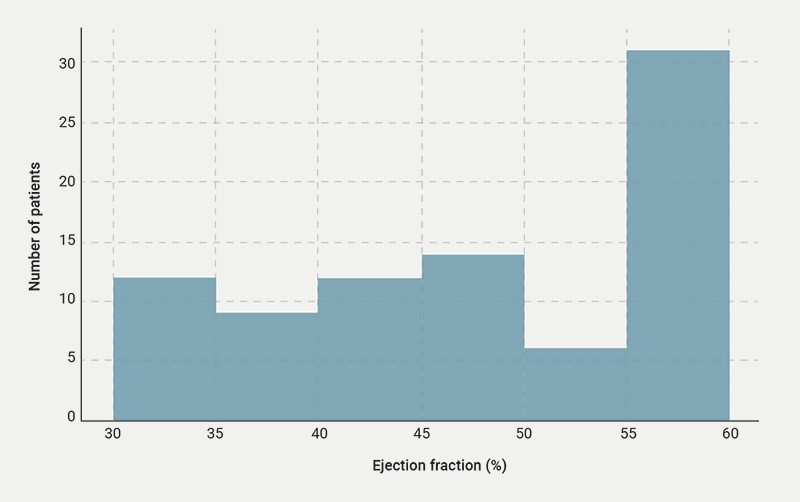
The average pre- and post-procedure QRS in the LBBAP group were 121.9 ms and 115.3 ms, respectively. In the HBP cohort it was 125.6 ms pre-procedure and 114 ms post-procedure. Of the patients with a broad QRS, 60% had left bundle-branch block (LBBB) and 40% had right bundle-branch block (RBBB). The distribution of LVEF can be seen in figure 2.
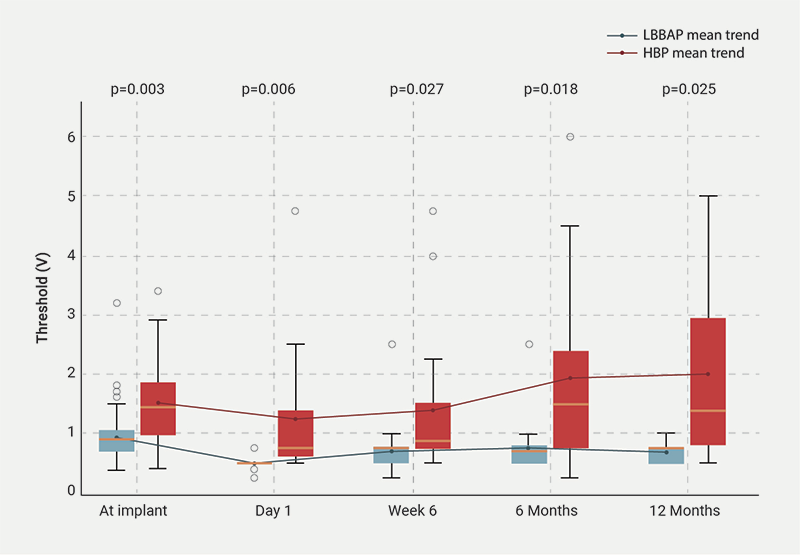
LBBAP demonstrated low and stable pacing thresholds throughout follow-up. The mean pacing threshold at implantation was 0.92 ± 0.44 V, which remained stable at subsequent follow-ups (0.69 ± 0.32 V at six weeks, 0.75 ± 0.37 V at six months, and 0.68 ± 0.19 V at 12 months). In contrast, HBP was associated with higher and more variable thresholds. The mean HBP threshold at implant was 1.51 ± 0.78 V, increasing progressively over time (1.39 ± 1.21 V at six weeks, 1.93 ± 1.62 V at six months, and 2.00 ± 1.55 V at 12 months) (table 1 and figure 3). When looking at these data on an individual level, no LBBAP patients demonstrated a rise in capture thresholds by >1.0 V by six months, compared with 5/14 of HBP implants (p=0.002).
Table 1. Comparison of left bundle-branch area pacing (LBBAP) and His-bundle pacing (HBP) thresholds over time
| LBBAP threshold, V | HBP threshold, V | p value | |
| Implant | 0.92 ± 0.44 | 1.51 ± 0.78 | 0.003 |
| Day 1 | 0.49 ± 0.10 | 1.24 ± 1.04 | 0.006 |
| Week 6 | 0.69 ± 0.32 | 1.39 ± 1.21 | 0.027 |
| 6 months | 0.75 ± 0.37 | 1.93 ± 1.62 | 0.018 |
| 12 months | 0.69 ± 0.19 | 2.00 ± 1.55 | 0.025 |
| Key: HBP = His-bundle pacing; LBBAP = left bundle-branch area pacing | |||
| Key: HBP = His-bundle pacing; LBBAP = left bundle-branch area pacing |
Lead impedance remained stable across both groups. For LBBAP, the mean implant impedance was 820.49 ± 271.80 Ω, and 429.55 ± 111.41 Ω at six months. HBP values were similar, with an implant impedance of 718.44 ± 203.32 Ω and 389.50 ± 91.80 Ω at six months (table 2). LBBAP also showed robust sensing performance, with high and stable R-wave amplitudes at implant (9.9 ± 5.48 mV), day 1 (10.52 ± 6.53 mV), six weeks (10.99 ± 6.94 mV), and six months (11.12 ± 6.92 mV). The mean implant LVAT was 82.6 ± 12.39 ms.
Table 2. Comparison of LBBAP and HBP impedance over time
| LBBAP impedance, Ω | HBP impedance, Ω | p value | |
| Implant | 820.49 ± 271.80 | 718.44 ± 203.32 | 0.103 |
| Day 1 | 547.83 ± 96.82 | 411.00 ± 81.65 | <0.001 |
| Week 6 | 484.68 ± 119.76 | 411.22 ± 91.70 | 0.009 |
| 6 months | 429.55 ± 111.41 | 389.50 ± 91.80 | 0.216 |
| 12 months | 355.57 ± 23.82 | 362.90 ± 71.90 | 0.770 |
| Key: HBP = His-bundle pacing; LBBAP = left bundle-branch area pacing | |||
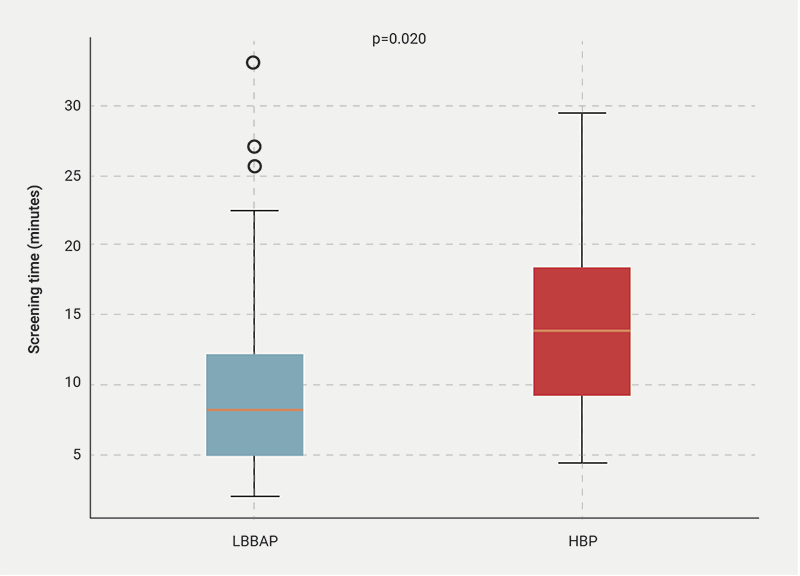
The HBP group had a slightly longer mean screening time (14.42 ± 7.31 minutes vs. 9.88 ± 6.53 minutes), which was statistically significant (p=0.02) (figure 4).
| Key: HBP = His-bundle pacing; LBBAP = left bundle-branch area pacing |
CSP appeared to be a safe procedure overall. There were no cases of device infection or septal haematoma. There have been no requirements for lead revision to date for the 71 LBBAP patients. Two patients in the HBP group underwent lead revision (hazard ratio [HR] 17.14, p=0.067); one was upgraded to LBBAP and the other was switched to single-chamber atrial (AAI) pacing. This finding suggests a trend towards higher lead revision risk with HBP, but did not reach statistical significance. One death occurred within 30 days of implant, but was not considered procedure related.
Nine patients (9.9%) were readmitted with HF across both groups during follow-up, occurring between 56 and 1,500 days post-implant. Follow-up echocardiograms were available for 15 patients: seven demonstrated either no change or an improvement in ejection fraction (EF), while eight showed a decline; post-procedure echo was performed based on clinical need, rather than specific protocol. These findings should be interpreted cautiously due to the small sample size and pre-existing HF in certain patients.
Discussion
This single-centre experience demonstrates that CSP can be effectively and safely implemented within a DGH setting. Our data reflect a growing confidence in the feasibility of CSP techniques outside tertiary centres, in line with broader trends in the UK and internationally.5,6
Consistent with existing literature, LBBAP was associated with lower and more stable pacing thresholds compared with HBP.3,4 This has significant clinical implications, as high or fluctuating thresholds in HBP can lead to battery depletion and the need for early generator replacement or lead revision. In contrast, LBBAP’s wider target zone within the interventricular septum allows for more consistent lead positioning and electrical capture, contributing to the stability observed. Our study also confirms that sensing parameters (R-wave amplitudes) with LBBAP are high and remain stable across follow-up.
In addition to electrical stability, the procedural ease of LBBAP plays a crucial role in its expanding use. Several studies have demonstrated that LBBAP implantation is associated with a shorter learning curve and a higher success rate, even in operators without prior CSP experience.7 This suggests that LBBAP may be particularly suitable for implementation in non-tertiary centres and supports its inclusion in contemporary pacing curricula.
There was a significantly shorter procedure time with LBBAP, compared with HBP, which may be due in part to the procedure being adopted later by operators with prior HBP experience; as well as the relative ease of lead placement in LBBAP. Standardised procedural practices, as outlined in the recent ‘Ten Commandments’ publication from the European Heart Rhythm Association (EHRA), are likely to further support efficiency and safety as CSP becomes more widely adopted.8
Our results are broadly consistent with the 2025 European Society of Cardiology (ESC) clinical consensus statement, which supports the use of CSP as a physiologically superior alternative to conventional pacing in a range of clinical scenarios.9 The consensus also encourages the incorporation of CSP into non-tertiary hospitals with appropriate training, procedural safeguards, and follow-up protocols. Recent studies, such as the His-SYNC and LBBP-RESYNC trials, have also compared CSP with biventricular pacing, highlighting the feasibility and physiological benefits of CSP in HF patients.10,11 Our observation of a small proportion of patients showing EF deterioration reinforces the need for larger, prospective trials to identify predictors of non-response to CSP.
From a healthcare systems perspective, CSP may offer cost advantages over cardiac resynchronisation therapy (CRT) due to shorter procedure times, less device complexity, and fewer lead-related complications.12 However, the upfront investment in training and fluoroscopy exposure must be acknowledged and optimised through continued operator education.
Limitations of this study include its retrospective, single-centre design and the relatively small sample size, particularly for follow-up echocardiographic data, which limits the generalisability of clinical outcome findings. Nonetheless, our findings are consistent with global trends and reinforce the feasibility of integrating CSP into everyday clinical practice.
Conclusion
Our experience at Chesterfield Royal Hospital demonstrates that conduction system pacing can be safely and effectively implemented within a DGH. These findings reinforce the procedural feasibility, electrical stability, and clinical safety of CSP in real-world practice. LBBAP, in particular, offered favourable pacing parameters and sensing performance, supporting its continued adoption as the preferred CSP modality. While challenges remain in terms of case selection and operator variability, CSP – especially LBBAP – is increasingly being positioned as the default strategy for patients requiring high ventricular pacing burden.
Future work should focus on identifying the patient subgroups most likely to benefit, understanding long-term outcomes beyond 12 months, and refining follow-up protocols to detect non-response early. As operator experience grows and national guidance evolves, ongoing training and standardised follow-up protocols will be essential to support the rapid expansion of CSP as an integral component of routine pacing strategies across all levels of hospital care. Ultimately, CSP has the potential to replace conventional RV pacing in the majority of patients, aligning cardiac pacing practice with modern standards of physiological therapy.
Key messages
- First district general hospital reporting head-to-head comparison of left bundle-branch area pacing (LBBAP) and His-bundle pacing (HBP)
- Comprehensive analysis of the feasibility of conduction system pacing (CSP) within a district general hospital setting
Conflicts of interest
None declared.
Funding
None.
Study approval
Ethical approval was not required.
References
1. Sharma PS, Naperkowski A, Bauch TD et al. Permanent His bundle pacing for cardiac resynchronisation therapy: a multicentre experience. Heart Rhythm 2018;15:413–20. https://doi.org/10.1016/j.hrthm.2017.10.014
2. Tops LF, Schalij MJ, Holman ER, van Erven L, van der Wall EE, Bax JJ. Right ventricular pacing can induce ventricular dyssynchrony in patients with preserved ejection fraction. J Am Coll Cardiol 2006;48:1642–8. https://doi.org/10.1016/j.jacc.2006.05.072
3. Vijayaraman P, Subzposh FA, Naperkowski A et al. Prospective evaluation of feasibility and electrophysiologic and echocardiographic characteristics of left bundle branch area pacing. Heart Rhythm 2019;16:1774–82. https://doi.org/10.1016/j.hrthm.2019.05.011
4. Huang W, Su L, Wu S et al. A novel pacing strategy with low and stable output: pacing the left bundle branch immediately beyond the His bundle. Can J Cardiol 2017;33:1736.e1–1736.e3. https://doi.org/10.1016/j.cjca.2017.09.013
5. Jastrzębski M, Kiełbasa G, Cano O et al. Left bundle branch area pacing outcomes: the multicentre European MELOS study. Eur Heart J 2022;43:4161–73. https://doi.org/10.1093/eurheartj/ehac445
6. Vijayaraman P, Ponnusamy SS, Cano Ó et al. Left bundle branch area pacing for cardiac resynchronization therapy: results from the International LBBAP Collaborative Study Group. JACC Clin Electrophysiol 2021;7:768–89. https://doi.org/10.1016/j.jacep.2020.08.015
7. Ponnusamy SS, Vijayaraman P. My preferred approach to left bundle branch pacing: lumenless leads. Heart Rhythm O2 2023;4:308–21. https://doi.org/10.1016/j.hroo.2022.12.012
8. Michowitz Y, Glikson M, Burri H. The ‘10 Commandments’ from the 2025 ESC/EHRA Clinical Consensus Statement on Indications for Conduction System Pacing (CSP). Eur Heart J 2025;46:2844–6. https://doi.org/10.1093/eurheartj/ehaf371
9. Glikson M, Burri H, Abdin A et al. European Society of Cardiology (ESC) clinical consensus statement on indications for conduction system pacing, with special contribution of the European Heart Rhythm Association of the ESC and endorsed by the Asia Pacific Heart Rhythm Society, the Canadian Heart Rhythm Society, the Heart Rhythm Society, and the Latin American Heart Rhythm Society. Europace 2025;27:euaf050. https://doi.org/10.1093/europace/euaf050
10. Upadhyay GA, Vijayaraman P, Nayak HM et al.; His-SYNC Investigators. His corrective pacing or biventricular pacing for cardiac resynchronization in heart failure. J Am Coll Cardiol 2019;74:157–9. https://doi.org/10.1016/j.jacc.2019.04.026
11. Wang Y, Zhu H, Hou X et al.; LBBP-RESYNC Investigators. Randomized trial of left bundle branch vs biventricular pacing for cardiac resynchronization therapy. J Am Coll Cardiol 2022;80:1205–16. https://doi.org/10.1016/j.jacc.2022.07.019
12. Vijayaraman P, Zanon F, Ponnusamy SS et al. Conduction system pacing compared with biventricular pacing for cardiac resynchronization therapy in patients with heart failure and mildly reduced left ventricular ejection fraction: results from International Collaborative LBBAP Study (I-CLAS) Group. Heart Rhythm 2025;22:1512–22. https://doi.org/10.1016/j.hrthm.2024.09.030
