We present a case involving the discovery of an extracardiac mass during a routine ablation procedure for typical atrial flutter. Using multiple imaging modalities it was possible to assess the mass during the procedure, leading to successful completion of the ablation.
Case
A 65-year-old man presented for an elective ablation for typical atrial flutter under general anaesthetic. Other than rivaroxaban 20 mg and bisoprolol 5 mg initiated two weeks prior, the patient was on no regular medication. The patient’s past medical history was significant for prostate cancer, for which he was awaiting prostatectomy, and pre-procedural work-up including bloods and physical examination were unremarkable. The patient was in atrial flutter with typical appearances at baseline.
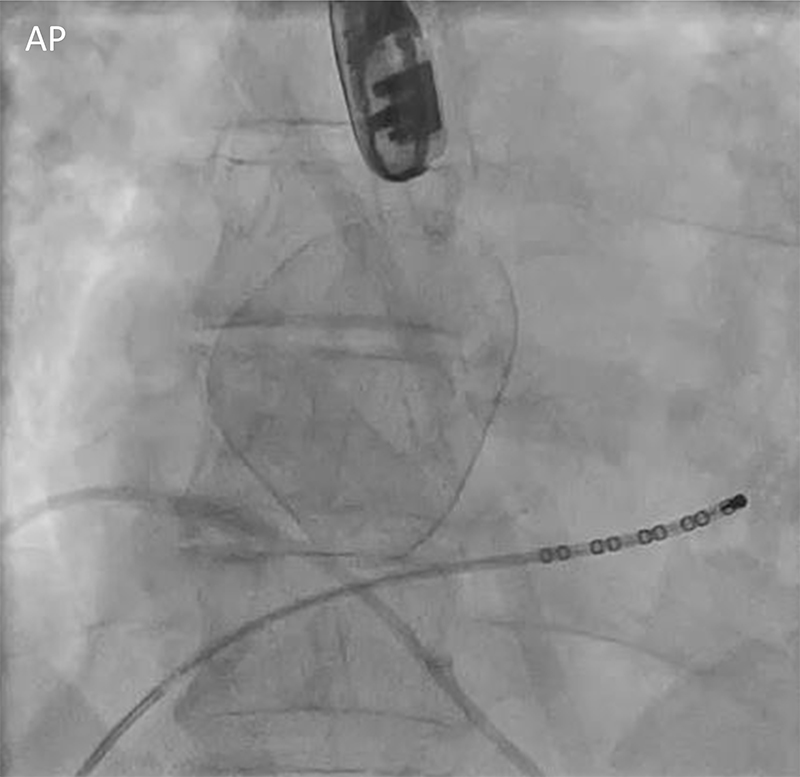
The procedure was performed under general anaesthetic with transoesophageal echo (TOE) to exclude thrombus in the left atrial appendage due to anticoagulation being initiated fewer than 28 days prior. Fluoroscopy during the procedure revealed a well-circumscribed, ovoid structure in the anterior mediastinum (figure 1). Orthogonal views revealed the mass lying anterior to the right atrium. Periprocedural TOE identified a fluid-filled mass adjoining the tricuspid annulus, without evidence of communication with the cardiac chambers with either bubble injection or Doppler flow. The 3D electroanatomic map created during the procedure (figure 2) (Carto 3, Johnson & Johnson, Laguna Hills, CA) showed a scalloped appearance of the right atrium, consistent with the position of the mass. There were normal voltage signals (>0.5 mV) throughout the atrium. The 3D map created indicated distortion of the tricuspid annulus, though valvular parameters, as assessed by TOE, were within normal ranges.
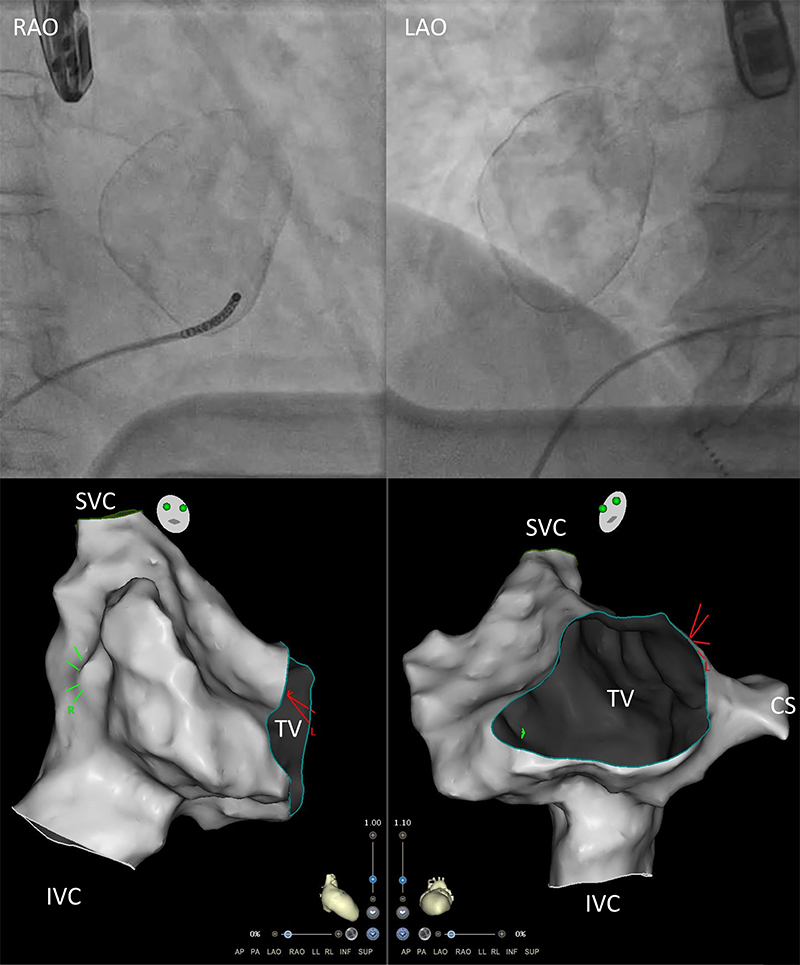
| Key: CS = coronary sinus; IVC = inferior vena cava; SVC = superior vena cava; TV = tricuspid valve |
Initially, there was concern that the mass could possibly represent a direct cardiac abnormality and, therefore, ablation in the vicinity of the mass may have a higher procedural risk attached. Consequently, there was discussion as to whether to postpone the ablation to allow its formal assessment, or if it was safe to proceed. The periprocedural assessment of the mass using TOE, fluoroscopy and electroanatomic 3D mapping, provided key information demonstrating that the mass was beyond the myocardial border and did not communicate with the blood pool. The 3D electroanatomic map, in particular, demonstrating a scalloped anterior right atrium (figure 2) was particularly helpful, as it provided direct visualisation of the relationship between the mass and the right atrium, and distance from the cavotricuspid isthmus, in the absence of cross-sectional imaging. The inability to pass mapping catheters to the area corresponding to the mass helped confirm that the mass did not communicate with the right atrium. The fluoroscopic appearance with a calcified rim, heavily suggested that this mass was a chronic incidental finding rather than an acute one. Distinguishing the structure from the valve annulus itself was challenging with echo alone, and was only achieved by using the 3D map.
Overall, with evidence to indicate chronicity of the lesion, no communication with the cardiac chambers, and a preserved cavotricuspid isthmus anatomy, it was determined that the procedure could be safely continued. The atrial flutter had a cycle length 220 ms, and entrainment from the cavotricuspid isthmus confirmed successful acceleration of the tachycardia, and a post-pacing interval of 230 ms confirming the tachycardia as typical atrial flutter. The cavotricuspid isthmus ablation was completed successfully and uneventfully with bidirectional block demonstrated. No pericardial effusion was seen on the end of procedure TOE.
Subsequent investigations included a triple-phase computed tomography (CT) and cardiac magnetic resonance imaging (MRI), which confirmed the presence of a non-communicating, calcified, fluid-filled structure lying in the anterior mediastinum. Its appearances across multiple imaging modalities were consistent with a pericardial cyst. The CT suggested possible mass effect compression of the right coronary artery, without significant change to luminal flow or distal opacification of the vessel (figure 3). The patient was asymptomatic of any anginal chest pain or other cardiac symptoms and, therefore, after review with the cardiothoracic team, it was decided for surveillance rather than surgical management of this cyst in the first instance.
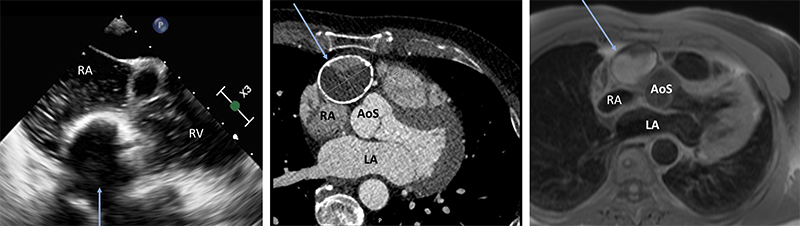
| Key: AoS = aortic ainuses; LA = left atrium; RA = right atrium; RV = right ventricle |
Discussion
Pericardial cysts are most commonly identified incidentally, and are usually congenital abnormalities. They are rare, occurring in approximately one in 100,000 patients, and common differentials include cystic teratomas and pericardial diverticulae.1 Intervention is usually only warranted if there are mass effects or symptoms. This case demonstrates how a 3D electrophysiology mapping system, which is usually used to identify the position of catheters within cardiac chambers and activation timing to allow mapping of arrhythmias, was helpful in the periprocedural assessment of the mass and its relationship to cardiac anatomy, and allowed the safe continuation of a procedure with significant anatomical variation. Although the local cavotricuspid anatomy was not distorted by the cyst in this instance, this is certainly a possibility in patients where cysts are identified. The use of 3D mapping here was key to confirm unaltered cavotricuspid anatomy and, therefore, facilitate a safe and uninterrupted procedure. Importantly, in a fluoroscopy free procedure workflow, the distortion of the tricuspid annulus and scalloped atrial appearances could help arouse suspicion of external compression, and may prompt further investigations to elucidate the cause. With significant anatomical variation, such as demonstrated in this case, normal fluoroscopic anatomical markers may be invalid, and this further highlights the importance of 3D mapping in such instances. The multi-modality imaging confirmed typical findings of a pericardial cyst and the patient had no previous cross-sectional imaging to compare. Electrocardiogram (ECG) markers that could be suggestive of a compressive mass, such as respiratory phase variations in cycle length, were absent.
Atrial flutter and other atrial arrhythmias have been associated with pericardial disease, in particular pericarditis.2–4 Although there were no signs of acute inflammation in this case (with a normal C-reactive protein and full blood count, and no imaging findings suggestive of acute inflammation), the pericardial pathology identified may indeed have been a contributing factor to the development of his atrial flutter. The pathophysiology of atrial arrhythmias in the context of pericarditis has not been established, but may possibly be due to pericardial inflammation in close proximity to atrial tissue. In this instance, localised pericardial pathology from the pericardial cyst may possibly have contributed to the development of atrial flutter, perhaps due to stretch and mechanical strain on pericardial and atrial tissue from the cyst. To our knowledge, this is the only case report where 3D mapping during atrial flutter ablation has helped to identify an extra-cardiac lesion.
Conflicts of interest
None declared.
Funding
None.
Patient consent
Written consent was obtained for the publication of this report.
References
1. Kar SK, Ganguly T. Current concepts of diagnosis and management of pericardial cysts. Indian Heart J 2017;69:364–70. https://doi.org/10.1016/j.ihj.2017.02.021
2. Spodick DH. Arrhythmias during acute pericarditis. A prospective study of 100 consecutive cases. JAMA 1976;235:39–41. https://doi.org/10.1001/jama.1976.03260270025020
3. Spodick DH. Frequency of arrhythmias in acute pericarditis determined by Holter monitoring. Am J Cardiol 1984;53:842–5. https://doi.org/10.1016/0002-9149(84)90416-8
4. Schwartz C, Khadilkar AC, Bitetzakis C, Patel A. A case of atrial flutter masking acute pericarditis. Cureus 2021;13:e14168. https://doi.org/10.7759/cureus.14168
