Whose problem is it?

NICE emphasises that public health and clinical audiences need complementary guidance to address the hazy divisions between prevention and management of obesity.3 This was stressed again in recent guidance.20
It is unlikely that the problems of obesity can be addressed through primary care management alone. NICE recognises that “the clinical management of obesity cannot be viewed in isolation from the environment in which people live”.3 Its recommendations have a broad scope covering:
- clinical management in primary and secondary care
- prevention in people who are currently a healthy weight, outside clinical settings
- developing local strategies, focused on interventions in:
– wider community services
– young children (aged 2–5 years)
– schools
– workplaces.
The role of the GP
So what is the role of the GP? According to the RCP and many other national organisations, GPs have a pivotal role to play in the prevention and management of overweight and obesity in adults. “Having a uniquely holistic view, each GP consultation provides the opportunity for advice on weight and, if necessary, prevention,” says the Royal College of Physicians (RCP) in its Action on obesity report.1
The National Obesity Forum considers obesity and overweight can be managed in primary care by a motivated well-informed multi-disciplinary team. The aim of treatment is to achieve and maintain weight loss by promoting sustainable changes in lifestyle.
Unfortunately, weight management and treatment is often carried out badly in primary care. It is not yet part of the Quality and Outcome Framework (QoF) although there have been many calls by national organisations (such as the RCP) for it to be included. The medical curriculum too is historically poor in this area and many GPs require, and want, further training.
The RCP recommends that obesity and behavioural change therapy become essential components of all training. It also emphasises core training in obesity management and prevention in general practice, which should continue throughout professional life.1 This has also been recommended recently by NICE.20 The RCP makes six recommendations for the role of the GP and general practice team in weight management (see table in drop down box).1
• The role of the GP and general practice team in weight management1
View details
All GPs should be in a position to adopt the following core approaches after training it says:1
- sensitively raise awareness of weight issues and impact on health
- understand the complexity of obesity and the need to leave judgmental attitudes behind
- undertake and convey metabolic risk assessment to patients
- use motivational approaches to help patients set relevant and feasible goals and balance this with the needs of other health promotion areas such as smoking
- be aware of local community services and bariatric care pathways and signpost patients to them
- targeted prevention of obesity or early manifestations of its metabolic impact (eg. pre-diabetes).
NICE has also reinforced this approach in their latest guidance.20 This includes recommendations that healthcare professionals should be aware of i) the local obesity pathway, ii) the range of local lifestyle weight management services available, iii) national sources of accurate information, iv) the continuing professional development or training opportunities available on weight management.
It is essential that GPs and other healthcare professionals work with local service providers to encourage an integrated approach to preventing and managing obesity.
Pivotal position
Primary care, including pharmacists, are at the frontline of obesity management being in contact with almost all overweight and obese individuals. Patients may present asking about ‘dieting’, or be attending diabetes or cardiovascular clinics as a result of their unhealthy weight but usually they will be at the surgery for something unrelated. Interacting with this latter group in a respectful and effective way is the first and most difficult part of managing obese patients for primary care. This process need only take the final two minutes of an unrelated consultation but it is crucial if obesity is to be addressed successfully.21

No obese person should be allowed to leave a consultation without their weight being addressed. Healthcare professionals are not only aware of the high risks associated with obesity, but are also able to help reduce these risks and offer treatments that are effective. If an obese patient’s weight can be measured, blood pressure assessed, blood tests organised and comprehensive follow-up assured, then a consultation has been successful. But, this is the start of an ongoing dialogue to motivate and support patients to engage in weight management. The initial phase of obesity management should be urgent correction of previously undiagnosed comorbidities, such as hypertension, dyslipidaemia or type 2 diabetes. Weight loss options can then be addressed. Whether weight is lost or not, the overall reduction in a patient’s global risk, however, should always be a focus of success.21
National guidance: NICE pathways
NICE guidance on the prevention, identification, assessment and management of overweight and obesity in children, young people and adults is expected to update its 2006 guidance later this year.3 A recent update has been given for its guidance on lifestyle weight management services for managing overweight and obesity in adults.20
Further guidance on management in children and young people has also been published by NICE in 201322 although this is outside the scope of this elearning module.
NICE 2006 guidance recommends:3
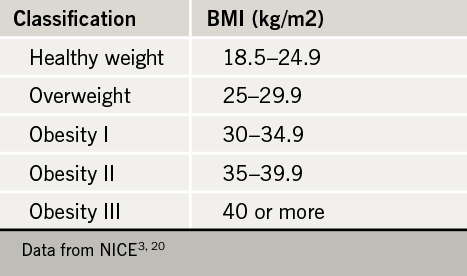
1. Determine degree of overweight or obesity
NICE recommends clinical judgment should be used to decide when to measure weight and height, and whether BMI or waist circumference should be measured. The latter should be used generally only if BMI < 35 kg/m2. A person should be told how these measurements affect their risk of long-term health problems (see measurement box, below)
Table 1 shows how to classify overweight and obesity using BMI.
Lower BMIs should be used as thresholds for concern in black African, African-Caribbean and Asian adults, where a BMI > 23 kg/m2 indicates an increasing risk of comorbidities, and a BMI of > 27.5 kg/m2 indicates a high risk. According to NICE, these groups may not be receiving health promotion advice when their BMI has reached these lower thresholds, which could create a significant health inequality.23 In older people, risk factors may be more important at higher BMIs. In highly muscular people, BMI is a less accurate indicator of adiposity.3
Table 2 shows waist circumference and risk. Waist circumference should generally only be used to indicate risk if BMI < 35 kg/m2. Waist circumference can be a better indicator of risk in some people, such as those of Asian descent24 (see measurement box, below).
