Practical issues associated with non-vitamin K antagonist oral anticoagulants (NOACs)
Laboratory measurement of anticoagulant effect
This is not required in routine use. It may, however, be useful in two situations:
- In bleeding patients, or those requiring urgent surgery, to estimate the amount of drug on board. The results of the basic clotting screen may be helpful here.
- To monitor anticoagulant effect in certain high-risk patient groups (extremes of body weight, renal impairment, interacting medications). This requires specialist assays.
Routine clotting tests and NOACs
When interpreting the results of screening clotting tests, it is useful to have the coagulation cascade in mind, Figure 4 shows the coagulation cascade, marked to show which bits are tested by the three screening clotting tests: PT (prothrombin time), APTT (activated partial thromboplastin time), and TT (thrombin time).
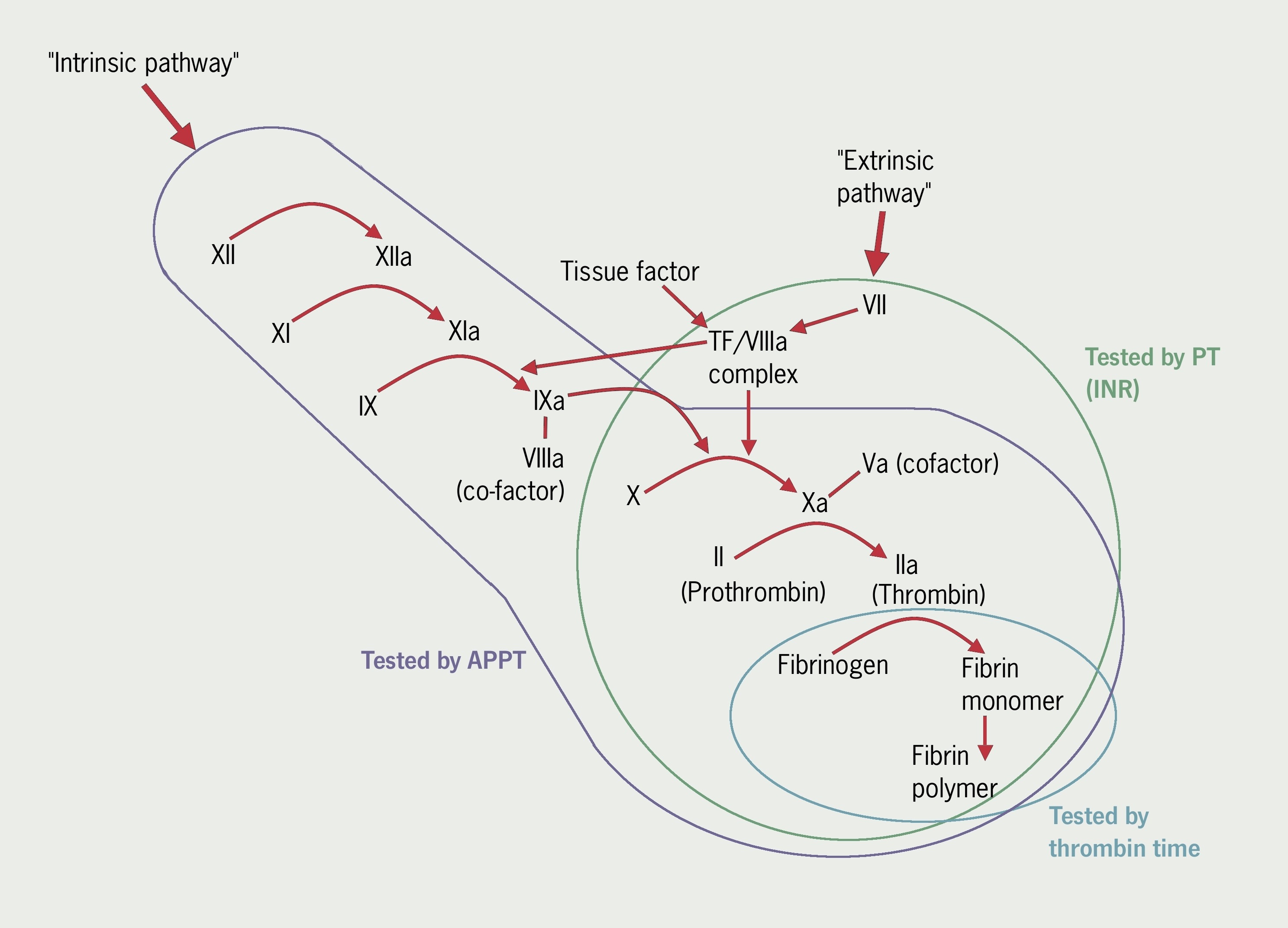
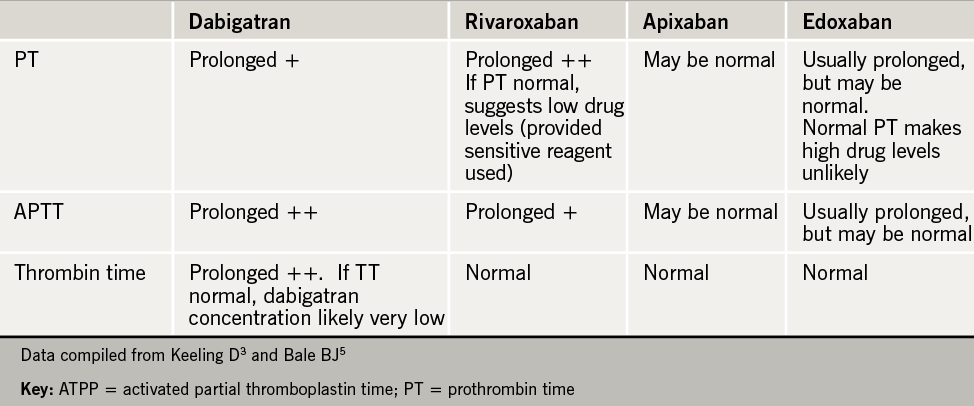
As might be predicted from figure 4, and a knowledge of the mechanism of action of NOACS, these anticoagulants may affect the results of screening clotting tests. However, results of these tests with NOACs are not consistent or standardised, and they therefore cannot be used for monitoring of these agents. Perhaps most importantly, results of standard clotting tests can be normal, even at therapeutic levels of anticoagulation with NOACS. Each lab will get different results depending on reagents, and results should be discussed with lab staff or a clinical haematologist. Table 4 is a guide showing the influence of NOACs on screening coagulation tests.3,5

For accurate measurement of drug levels, specialist assays have been developed (table 5). These may not be available in all laboratories.
Cessation of NOACs before invasive procedures
This is a confusing area. The manufacturers of each of the NOACs give recommendations, but pharmacokinetic modelling suggests that longer may be needed, especially in patients with impaired renal function, and where ensuring adequate haemostasis is crucial. Bridging anticoagulation with low molecular weight heparin is not usually necessary, but might be considered in certain high-risk situations. As ever, decisions should be individualised based on thrombotic and bleeding risk, and specialist advice sought. Table 6 is a guide.
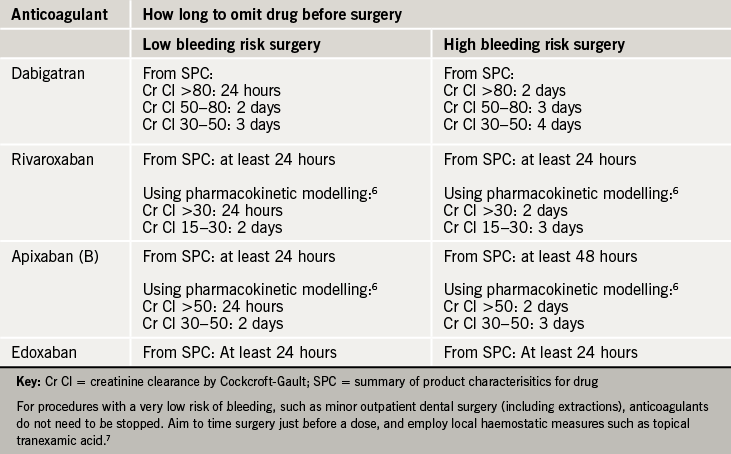
Recommendations on drug intake before surgery have also been issued by the European Heart Rhythm Association.8
close window and return to take test
References
1. Patient safety alert 18. National Patient Safety Agency 2007. Available from http://www.npsa.nhs.uk/nrls/alerts-and-directives/alerts/anticoagulant/ (accessed 20/02/13)
2. Oral anticoagulant therapy patient information booklet. National Patient Safety Agency 2008. Available from http://www.nrls.npsa.nhs.uk/resources/?EntryId45=61777 (accessed 20/02/13)
3. Keeling D, Baglin T, Tait C et al. British Committee for Standards in Haematology Guidelines on oral anticoagulation with warfarin – fourth edition. Br J Haematol 2011;154:1365–2141. http://dx.doi.org/10.1111/j.1365-2141.2011.08753.x
4. Tait RC, Sefcick A. A warfarin induction regimen for out-patient anticoagulation in patients with atrial fibrillation. Br J Haematol 1998;101:4504. http://dx.doi.org/10.1046/j.1365-2141.1998.00716.x
5. Dale BJ, Chan NC, Eikelboom JW. Laboratory measurement of the direct oral anticoagulants. Br J Haematol 2015 (published online 22nd October 2015). http://dx.doi.org/1111/bjh.13810
6. Spyropoulos AC, Douketis JD. How I treat anticoagulated patients undergoing an elective procedure or surgery. Blood 2012;120:2954−2962. http://dx.doi.org/10.1182/blood-2012-06-415943
7. National Institute for Health and Care Excellence. NICE Clinical Knowledge Summaries. Anticoagulation – oral. Available at http://cks.nice.org.uk/anticoagulation-oral (Accessed 5th November 2015)
8. Heidbuchel H, Verhamme P, Alings M, et al. Updated European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist anticoagulants in patients with non-valvular atrial fibrillation. Europace 2015;17:1467–507. http://dx.doi.org/10.1093/europace/euv309
Further reading
Hicks T, Stewart F, Eisinga A. NOACs versus warfarin for stroke prevention in patients with AF: a systematic review and meta-analysis. Open Heart 2016;3:e000279. http://dx.doi.org/10.1136/openhrt-2015-000279
close window and return to take test
All rights reserved. No part of this programme may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without the prior permission of the publishers, Medinews (Cardiology) Limited.
It shall not, by way of trade or otherwise, be lent, re-sold, hired or otherwise circulated without the publisher’s prior consent.
Medical knowledge is constantly changing. As new information becomes available, changes in treatment, procedures, equipment and the use of drugs becomes necessary. The editors/authors/contributors and the publishers have taken care to ensure that the information given in this text is accurate and up to date. Readers are strongly advised to confirm that the information, especially with regard to drug usage, complies with the latest legislation and standards of practice.
Healthcare professionals should consult up-to-date Prescribing Information and the full Summary of Product Characteristics available from the manufacturers before prescribing any product. Medinews (Cardiology) Limited cannot accept responsibility for any errors in prescribing which may occur.
