Aortic dilatation is more likely with associated coarctation, but dissection is relatively uncommon and has a relatively high operative success, probably because of the youth and underlying good health of the subject. Prophylactic surgery is necessary in about 5% during a 20-year follow-up.
Vasculitides, especially giant-cell arteritis and Takayasu’s arteritis may weaken the arterial wall. Other causes of aortic dilatation are trauma, cocaine and amphetamines.
Acute aortic regurgitation occurs also as a result of endocarditis, dissection or trauma.
Mitral valve disease
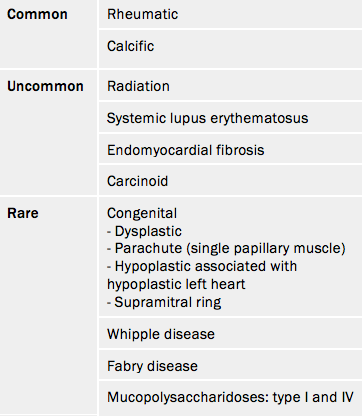
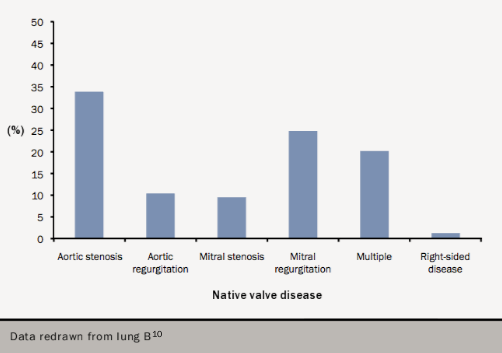
Rheumatic disease is the overwhelming aetiology world-wide (table 6) and causes isolated mitral stenosis in 40% of cases. However the population prevalence of mitral stenosis in the USA is only 0.1%10 and accounts for only 10% of cases in European hospital-based series.10
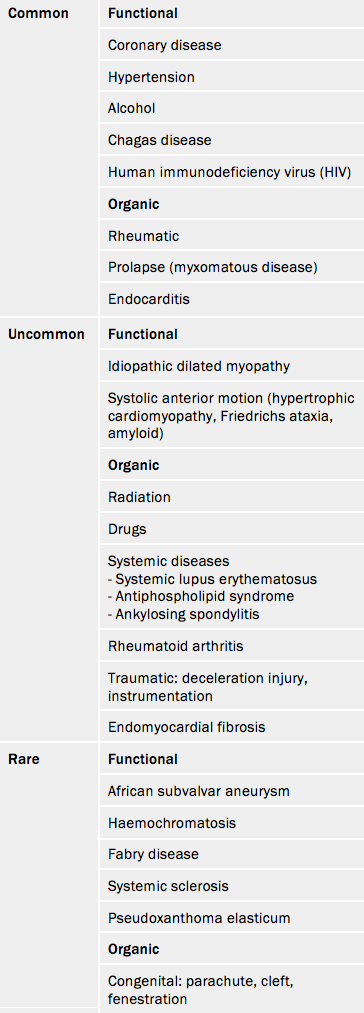
The mitral valve apparatus consists of leaflets, annulus, chordae and papillary muscles. Malfunction of one or more of these components can cause mitral regurgitation. Mitral regurgitation is categorised as organic if caused by primary valve dysfunction, and functional if secondary to left ventricular (LV) dysfunction. In the industrialised countries or in the elderly elsewhere, mitral regurgitation (table 7) is predominantly functional, secondary to LV dysfunction.
The cause of LV dysfunction leading to functional mitral regurgitation reflects the causes of heart failure which vary geographically. Endomyocardial fibrosis (EMF) is the second most frequent cause of acquired heart disease in children and young adults in equatorial Africa16 with a prevalence of 20% in coastal Mozambique.
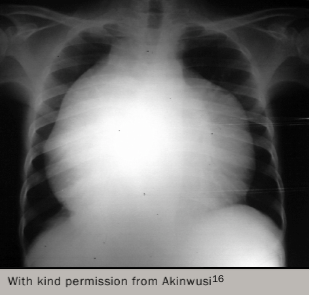
EMF is an idiopathic disease that is mostly confined to the tropical and subtropical rainforest regions of the world. However, subsequent reports have shown its occurrence in the guinea savannah of Nigeria, and even outside the tropical zones. It is the most common cause of restrictive cardiomyopathy worldwide. The disease causes fibrosis of the endocardium, leading to impaired filling. The right ventricle is the most commonly affected, followed by biventricular and then left ventricular involvement. Figure 1117 shows a young patient with EMF, who has New York Heart Association Class III disease necessitating hospital admission to stabilise.
EMF begins as a febrile illness followed by a latent phase of 2–10 years. Symptoms then reappear as LV and right ventricular (RV) thrombi and fibrosis develop leading to RV, LV or biventricular restrictive cardiomyopathy and encasement of the mitral or tricuspid valves. The pathology of EMF is still uncertain.
Mitral prolapse occurs in 2% in Western populations with significant regurgitation in about 9% of these. In the USA the population prevalence is 1.7%1 while mitral regurgitation represented 32% of a hospital-based European survey.10
Congenital mitral disease is uncommon. Patterns described in a series of 49 autopsy cases of congenital mitral stenosis were:
- dysplastic;
- parachute (single papillary muscle);
- hypoplastic associated with hypoplastic left heart;
- supramitral ring.
Right-sided valve disease
Right-sided disease is uncommon, occurring in 1.2% in the EuroHeart Survey.10 It was not mentioned in USA population-based studies.
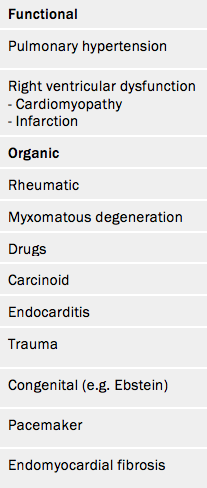
Tricuspid stenosis (see table 8) is almost always rheumatic and associated with left-sided disease. Tricuspid regurgitation is commonly functional as a result of pulmonary hypertension or right ventricular myopathy or infarction (see table 9).
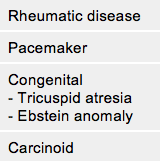
Pulmonary regurgitation is commonly functional as a result of pulmonary hypertension (see table 10). Either stenosis or regurgitation occurs in approximately 14% of all congenital cardiac lesions.
Multiple valve disease
Multiple valve involvement represented a significant subgroup in the EuroHeart Survey and occurred in 20% of the database (see figure 12).10 The causes of multiple valve involvement include:
- rheumatic disease
- myxomatous disease
- endocarditis
- drugs
- carcinoid
- radiation.
Conclusion
Valve disease is correctly regarded as an epidemic ‘waiting to happen’.17 Degenerative aortic stenosis has become the most common valve disease in Europe, and the United States, due to prolonged life-expectancy and the associated degenerative effects on cardiac structures. In this module, we have looked at other forms of valve disease, particularly those related to rheumatic fever, which continues to be a public health challenge in the developing world.
Other modules in this programme will take us forward into looking at the underlying causes of heart valve disease, along with its presentation, diagnosis and treatment.
Key messages
- Rheumatic disease is the most common cause of valve disease in the young worldwide with an estimated prevalence of 15.6–19.6 million
- In industrially developed regions diseases of old age predominate, particularly calcific aortic stenosis and functional mitral regurgitation
- In the USA, valve disease is most common in the elderly with a prevalence of 13% in those aged over 75
- Drug-induced valve disease is increasing as a result of 5HT2b receptor agonists
- Infective endocarditis is increasingly related to medical devices and intravenous drug use
- Failure of biological replacement valves is a major burden in all regions of the world
- Variations in access to care exist across the world but also within individual countries

References
1. Nkomo VT, Gardin JM, Skelton TN, et al. Burden of valvular heart diseases: a population-based study. Lancet 2006;368:1005–11. http://dx.doi.org/10.1016/S0140-6736(06)69208-8
2. Carapetis JR. Rheumatic heart disease in developing countries. New Engl J Med 2007;357:439. http://dx.doi.org/10.1056/NEJMp078039
3. Soler-Soler J, Galve E. Worldwide perspective of valve disease. Heart 2000;83:721–5. http://dx.doi.org/10.1136/heart.83.6.721
4. Fox DJ, Khattar RS. Carcinoid heart disease: presentation, diagnosis, and management. Heart 2004;90:1224–8. http://dx.doi.org/10.1136/hrt.2004.040329
5. Grunkemeier GL, Li H-H, Naftel DC, Starr A, Rahimtoola SH. Long-term performance of heart valve prostheses. Curr Prob Cardiol 2000;25:73–156. Available from: http://www.cpcardiology.com/article/PIIS0146280600000244/fulltext
6. Zilla P, Brink J, Human P, Bezuidenhout D. Prosthetic heart valves: catering for the few. Biomaterials 2008;29:385–406. http://dx.doi.org/10.1016/j.biomaterials.2007.09.033
7. Bridgewater B, Kinsman R, Walton P et al. Demonstrating quality: the sixth National Adult Cardiac Surgery database report. Henley on Thomas UK. Dendrite Clinical Systems Ltd, 2009.
8. Habib G, Hoen B, Tornon P et al. Guidelines on the prevention, diagnosis, and treatment of infective endocarditis. Eur Heart J 2009;30:2369–413. http://dx.doi.org/10.1093/eurheartj/ehp285
9. Otto CM, Bonow RO. Valvular heart disease: a companion to Braunwald’s heart disease – expert consult. Saunders; 3rd edition 2009.
10. Iung B, Baron G, Butchart EG, et al. A prospective survey of patients with valvular heart disease in Europe: the Euro Heart Survey on Valvular Heart Disease. Eur Heart J 2003;24:1231–43. http://dx.doi.org/10.1016/S0195-668X(03)00201-X
11. Lindroos M, Kupari M, Heikkala J, Tilvis R. Prevalence of aortic valve abnormalities in the elderly: an echocardiographic study of a random population sample. J Am Coll Cardiol 1993;21:1220–5. http://dx.doi.org/10.1016/0735-1097(93)90249-Z
12. Nistri S, Basso C, Marzari C et al. Frequency of bicuspid aortic valve in conscripts by echocardiogram. Am J Cardiol 2005;96:718–21. http://dx.doi.org/10.1016/j.amjcard.2005.04.051
13. Michelena HI, Desjardins VA, Avierinos J-F, et al. Natural history of asymptomatic patients with normally functioning or minimally dysfunctional bicuspid aortic valve in the community. Circulation 2008;117:2776–84. http://dx.doi.org/10.1161/CIRCULATIONAHA.107.740878
14. Lebowitz NE, Bella JN, Roman MJ et al. Prevalence and correlates of aortic regurgitation in American Indians: The Strong Heart Study. J Am Coll Cardiol 2000;36:461–7. http://dx.doi.org/10.1016/S0735-1097(00)00744-0
15. Mocumbi AO, Yacoub S, Yacoub MH. Neglected tropical cardiomyopathies: II Endomyocardial fibrosis: Myocardial disease. Heart 2008;94:384–90. http://dx.doi.org/10.1136/hrt.2007.136101
16. Akinwusi PO, Odeyemi AO. The changing pattern of endomyocardial fibrosis in South-West Nigeria. Clin Med Insights: Cardiol 2012;6:163–8. http://dx.doi.org/10.4137/CMC.S10141
17. d’Arcy JL, Prendergast BD, Chambers JB, Ray SG, Bridgewater B. Valvular heart disease: the next cardiac epidemic. Heart 2011;97:91–3. http://dx.doi.org/10.1136/hrt.2010.205096
Suggested further reading
Chambers J. Heart valve disease introduction. Int J Clin Prac 2014;68:1179–80. http://onlinelibrary.wiley.com/doi/10.1111/ijcp.12224/epdf
Rayner J, Coffey S, Newton J, Prendergas BD. Aortic valve disease. Int J Clin Prac 2014;68:1209–15. http://onlinelibrary.wiley.com/doi/10.1111/ijcp.12471/epdf
Coffey S, Rayner J, Newton J, Prendergast BD. Right-sided valve disease. Int J Clin Prac 2014;68:1221–6. http://onlinelibrary.wiley.com/doi/10.1111/ijcp.12485/epdf
close window and return to take test
All rights reserved. No part of this programme may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without the prior permission of the publishers, Medinews (Cardiology) Limited.
It shall not, by way of trade or otherwise, be lent, re-sold, hired or otherwise circulated without the publisher’s prior consent.
Medical knowledge is constantly changing. As new information becomes available, changes in treatment, procedures, equipment and the use of drugs becomes necessary. The editors/authors/contributors and the publishers have taken care to ensure that the information given in this text is accurate and up to date. Readers are strongly advised to confirm that the information, especially with regard to drug usage, complies with the latest legislation and standards of practice.
Healthcare professionals should consult up-to-date Prescribing Information and the full Summary of Product Characteristics available from the manufacturers before prescribing any product. Medinews (Cardiology) Limited cannot accept responsibility for any errors in prescribing which may occur.
