Bicuspid aortic valve
Natural history
There are two large studies of the natural history of bicuspid aortic valve disease (BAV).48–9
During a 20 year follow-up, 24% of patients with a bicuspid aortic valve developed severe stenosis or regurgitation requiring surgery.48 Events were far more common in those with even mild valve thickening at baseline, with surgical rates of 75% at 12 years in the presence of thickening compared with only 8% without thickening.48
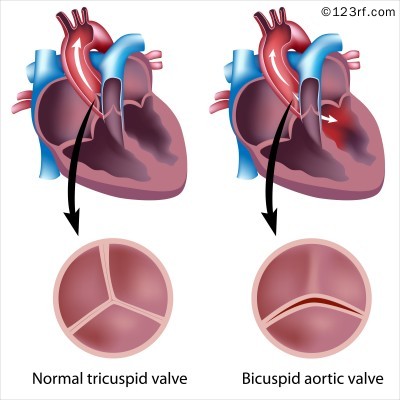
BAV (see figure 6) should be regarded as a general thoracic aortopathy and is associated with significant dilatation of the aorta to >40 mm as a result of medial necrosis50 in about 20% of cases,49 approximately one half affecting the root and the other the ascending aorta. Aortic dilatation is more likely with associated coarctation, but dissection is relatively uncommon and has a relatively high operative success probably because of the youth and underlying good health of the subject. Prophylactic aortic surgery is necessary in about 5% during a 20 year follow-up.48
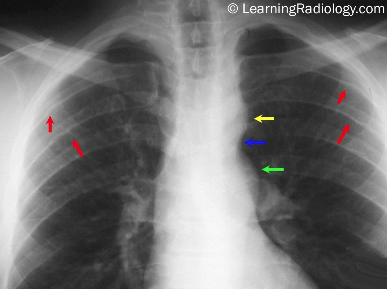
BAV may be associated with other congenital abnormalities and syndromes, most commonly coarctation of the aorta (see figure 7). The most common pattern, in 80% of cases, is failure of right-left separation which is more likely to be associated with aortic dilatation.51 Failure of separation of right and non-coronary cusps is more likely to be associated with mitral prolapse.51
Atherosclerosis risk factors are associated with progression of AS with BAV as well as calcific stenosis notably smoking and high cholesterol.52–54
Aortic regurgitation associated with BAV may result from annular dilatation of the aortic root due to aortic dilatation or dissection, as well as from the valve itself.
BAV is the commonest cause of valve replacement for AR, and tends to result in valve replacement earlier in life than with BAV AS. It has been shown that 15–20% of BAV will require valve replacement for AR.55 When AS and AR co-exist in BAV disease, AR is usually only mild or moderate in severity.
Exact figures for the incidence and prevalence of endocarditis on BAV are unknown, but case series have reported incidences of 10–30%.56 The population risk has been reported as lower than this however, at closer to 3%,57 although cusp perforation resulting from endocarditis causes up to 60% of AR in BAVs.56 In the context of BAV, endocarditis requires surgical intervention in a greater proportion of patients than endocarditis on a tricuspid aortic valve.58
Summary
- BAV disease may be associated with AS, AR or both
- Although valvular dysfunction is most commonly slowly progressive, it tends to result in symptoms, and require intervention, at an earlier age than disease of trileaflet aortic valves
- A systolic click may be the only sign of a normally-functioning BAV, but signs are otherwise similar to those of trileaflet valve dysfunction.
