Mitral stenosis (MS)
Natural history
Rheumatic involvement usually follows untreated recurrent rheumatic fever in childhood (see module 1 on epidemiology).
The normal mitral orifice is 4–5 cm2 in area and symptoms do not occur until the orifice area falls to below about 2.0 cm2. The rate of haemodynamic progression may be slow in two thirds of patients with wide variability between 0.1–0.3 cm2 per year.59-61 In those with more calcified and deformed valves, the decrease in orifice area may be as high as 0.3 cm2 per year.62
Like other forms of valve disease, MS in Western countries has a long asymptomatic period, which is associated with a good prognosis: 80% survival over a 20-year period. However, around half of patients will become symptomatic after 10 years.63 The five year survival with severe symptomatic MS was 44% without surgery.64
Pulmonary pressures are raised in MS initially by passive back-pressure and reactive vasoconstriction. Ultimately histological changes occur similar to those seen in primary pulmonary hypertension and these are irreversible.65
The left ventricle is protected since it is downstream from the valve lesion. However the right ventricle is under threat as pulmonary artery pressure rises. Established right heart failure as a result of pulmonary hypertension may cause a reduction in breathlessness as a result of lowered left atrial filling pressures. However this apparent improvement is spurious and a sign of end-stage and usually inoperable disease. MS can be seen in figure 8.
Symptoms may be precipitated by intercurrent illness, pregnancy or the development of atrial fibrillation. Clinical deterioration may be sudden in up to 50% of patients, and once symptoms are manifest, prognosis worsens. Heart failure is the cause of death in approximately 60%, with thromboembolic complications resulting in approximately 20% of deaths.66
Symptoms
The definition of severity in MS in particular is based on symptomatic onset and the severity at which intervention will improve symptomatic status. The most common symptom is exertional breathlessness as a result of raised left atrial pressure and fatigue as a result of low cardiac output.63 Exertional breathlessness is usually of slow onset so that the patient may claim to be asymptomatic. If there is any doubt, the patient should be exercised either formally or by simply walking with him or her in a hospital corridor.
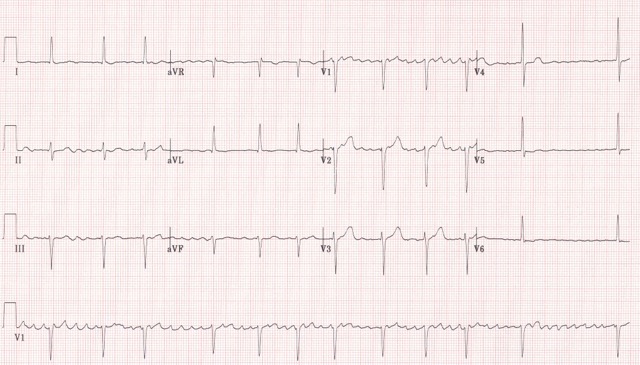
Episodic shortness of breath may be suggestive of paroxysmal atrial fibrillation (see figure 9), and can occur in the setting of fever and stress. Onset of atrial fibrillation may cause an acute deterioration in breathlessness.
Orthopnoea and paroxysmal nocturnal dyspnoea are caused by increased venous return on lying down leading to higher LV filling pressures and stiffening of the lungs.
The risk of thromboembolism in the presence of atrial fibrillation and MS is 18 times that of age-matched subjects67 and stroke may be the presenting symptom.
Complications of chronically raised pulmonary venous pressure are recurrent chest infections and, less commonly, haemoptysis. Dysphagia as a result of compression from a large left atrium and hoarseness from recurrent laryngeal nerve palsy occur rarely.
