Aortic regurgitation
Minimum echocardiographic dataset
The echocardiographic minimum dataset for aortic regurgitation consists of:
- appearance of the valve to detect aetiology
- colour mapping at the valve and in the arch
- spectral Doppler
- LV geometry and function
- aortic diameter.
Grading aortic regurgitation (see table 3)
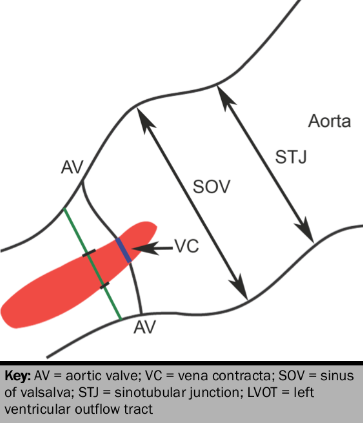
Colour Doppler jet width is quantified from the vena contracta width, and the height of the aortic regurgitation jet to the left ventricular outflow tract (LVOT) diameter (see figure 9).24
Continuous wave signal
The pressure half time (T1/2) is dependent on the LV diastolic pressure, and LV compliance as well as the grade of aortic regurgitation.25 A short pressure T1/2 can be caused either by severe regurgitation or LV dysfunction. The cut-point for severe regurgitation is therefore uncertain. Although a value of <200 ms is generally taken to imply severe aortic regurgitation, a value <300 is more sensitive, while a value >500 ms indicates mild regurgitation.
Flow reversal
A useful method for confirming the presence of severe aortic regurgitation is the assessment of flow within the proximal descending aorta. The detection of pandiastolic flow reversal with an end diastolic flow velocity of >20 cm/s is a sensitive sign of significant aortic regurgitation.26
Additional quantification
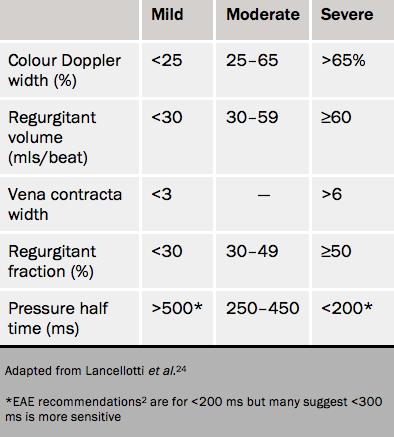
Other methods used are the regurgitant volume and also regurgitant fraction by either pulsed Doppler or by the proximal isovelocity surface area method. A regurgitant volume of ≥60 mls and a regurgitant fraction of ≥50% are taken to be indicative of severe aortic regurgitation.1
The rest of the heart
Left ventricle
With chronic volume load, the LV dilates. Ultimately, increased wall stress encourages subendocardial fibrosis with a fall in contractility and rise in end-systolic volume. Criteria for surgery include:
- LV end diastolic volume index ≥45 ml/m1,27
- LV end diastolic diameter of >70 mm
- LV systolic diameter of >50 mm (or 25mm/m2)
- LV ejection fraction (LVEF) of <50%.9
Advanced echocardiography
Strain and tissue Doppler imaging have also been proposed as markers of subclinical LV impairment but are not in routine clinical use. There is no clear role for stress echocardiography in aortic regurgitation, although evaluation of symptoms and assessment of LV contractile response to exercise may provide useful insight.
Cardiac computed tomography in aortic regurgitation
The role of cardiac computed tomography angiography (CTA) in the assessment of aortic regurgitation is limited (see table 2). It can help in assessing:
- the degree of leaflet malcoaptation on cardiac CT, which has been shown to have a sensitivity of 95% and specificity of 95–100% for the detection of moderate-severe aortic regurgitation when compared to TOE as a gold standard28
- aortic root anatomy and size in relation to the aortic valve
- It is technically feasible to also measure aortic regurgitant volumes and fractions. This is not routinely performed nor recommended, owing to the inability to exclude other concomitant valvular lesions, and the reliance on automated left and right ventricular segmentation to derive the relevant stroke volumes.
Cardiac magnetic resonance in aortic regurgitation
Aortic regurgitation is identified by diastolic reverse flow into the LVOT on SSFP cine imaging in the 3-chamber/LVOT view.
Accurate quantification of regurgitant volume and fraction can be obtained using in-plane flow imaging that is able to measure both the forward flow and the regurgitant flow across the aortic valve. Care needs to be taken with careful tracing around the area of interest of each frame of the cardiac cycle and the selection of the correct plane at which to measure flow,29 but the technique is then highly reproducible.30
There is evidence that regurgitant fraction by CMR better predicts risk than echo measures.31 It is also possible that serial LV volumes by CMR will be a better guide to the timing of surgery than linear dimensions by echo. This is because the LV becomes more spherical in the presence of severe aortic regurgitation and a serial linear dimension therefore becomes less reliable as a measure of change.
