Mitral regurgitation
A number of small studies with pre-clinical endpoints have demonstrated beneficial effects of beta blockers in chronic mitral regurgitation (MR).24,25 The trial with the longest duration of treatment randomised 38 patients with moderate to severe MR to metoprolol succinate or placebo and found that treatment protected against the worsening of LVSD seen in the placebo group.25
Similarly, a meta-analysis of trials examining ACEIs and ARBs in patients with MR and a normal ejection fraction found a reduction in regurgitant fraction in both randomised and non-randomised trials.26 However, larger trials with clinical endpoints are awaited before beta-blockers, ACEIs or ARBs can be recommended for routine use in patients with chronic MR and normal ejection fraction.
In patients with acute MR and heart failure, diuretics and nitrates are recommended to reduce filling pressure, while vasodilators are recommended to reduce afterload. Likewise, in patients with chronic MR and LVSD, treatment with diuretics, ACEIs or ARBs, beta blockers and aldosterone antagonists should be considered. Functional MR due to ventricular remodelling often improves with these therapies, or with cardiac resynchonisation therapy (CRT) (see figure 5), if other appropriate indications exist.
A rhythm control strategy for AF is rarely successful in patients with severe MR who are not undergoing surgical treatment.
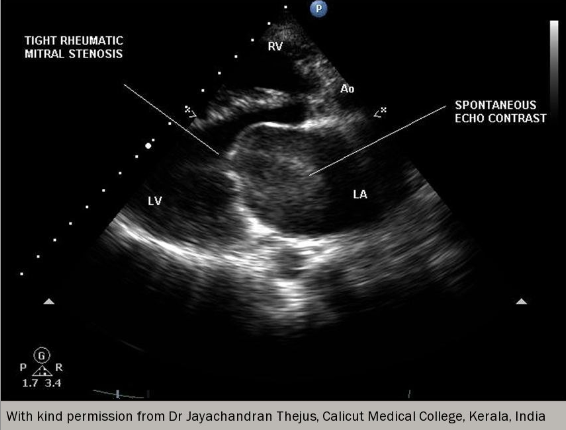
Mitral stenosis
In regions where rheumatic fever is endemic, secondary prevention is indicated as disease-modifying therapy in the majority of younger patients with mitral stenosis (MS) (see figure 6).27 Treatment should be with penicillin for 10 years or until 40 years of age (whichever is the longer) and life-long treatment should be considered for high-risk groups.