Chronic heart failure
Although some patients with fluid retention are thought of as having chronic heart failure, particularly if they do not actually need to be hospitalised, the term is best reserved for patients with treated acute heart failure.
Successful treatment of acute heart failure results in patients entering a chronic disease state: they usually have some degree of exercise limitation, but where it is well treated, do not have congestion and oedema.
Chronic heart failure is iatrogenic in the sense that before modern therapies were available, acute heart failure had a very bleak prognosis. Diuretics and treatment with neurohormonal antagonists allows chronic heart failure to develop.
Symptoms: The cardinal symptom of chronic heart failure is exercise limitation. Patients complain of breathlessness or fatigue on exertion, with the dominant symptom varying with the kind of exercise performed. The origin of symptoms is not clear.
Haemodynamics: In most patients with chronic heart failure, remodelling causes progressive dilation of the left ventricle. Stroke volume is maintained by an increase in left ventricular wall tension by the law of Laplace.
Cardiac output is usually normal at rest and during submaximal exercise, but may not be able to rise normally during more strenuous activity. However, there is little relation between haemodynamic variables, particularly when measured at rest, and exercise capacity.
Neurohormonal activation: The insight that many neurohormonal systems are activated in chronic heart failure has been the key to the success of modern medical therapy for heart failure:
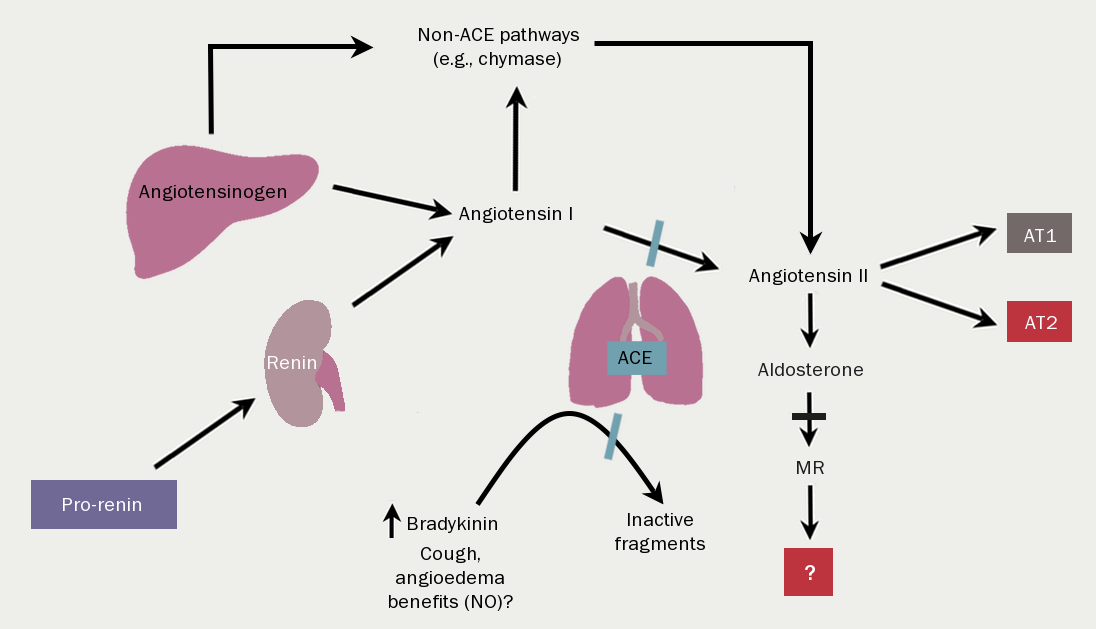
The renin-angiotensin-aldosterone system (RAAS) (figure 11) is activated by reduced renal perfusion. With worsening NYHA class symptoms, so the concentrations of angiotensin and aldosterone rise. Of note, the introduction of diuretic therapy results in further RAAS activation. The consequences are, inter alia, vasoconstriction, salt and water retention, increased vascular fibrosis and a positive interaction with…
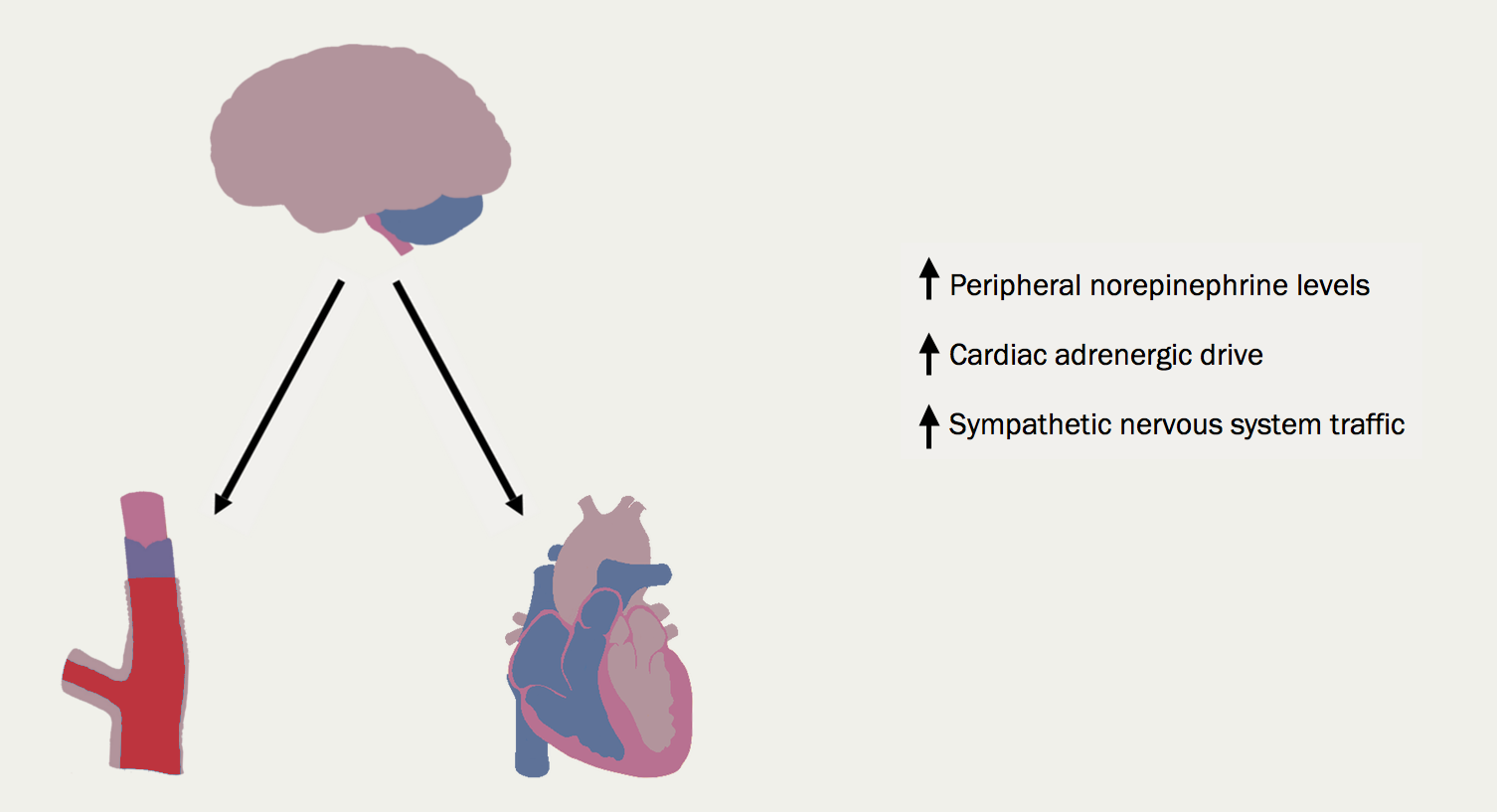
The sympathetic nervous system (figure 12). With worsening heart failure, so sympathetic nervous system activation and concentrations of circulating noradrenaline increase. The consequences for the heart include tachycardia, myocardial fibrosis and apoptosis, increased risk of arrhythmia and peripheral vasoconstriction (figure 13).

Natriuretic peptide concentrations rise as a homeostatic response to dilation of the cardiac chambers. Antidiuretic hormone (arginine vasopressin) is also increase, further enhancing water retention.
Other hormone systems are activated, although their clinical relevance is not always clear. The potent vasoconstrictor, endothelin, is raised, and more intriguingly, there is activation of components of the immune system, with increases in tumour necrosis factor and c-reactive protein, for example.
Skeletal muscle changes: these can be very prominent in some patients resulting in cachexia, but almost all patients have some degree of loss of lean muscle bulk. The skeletal muscle changes correlate closely with impaired exercise capacity, and appear to be implicated, at least in part, as the cause of sympathetic nervous system activation.
Peripheral changes: these include the down-regulation of baroreceptors (making them unlikely to be the source of sympathetic nervous system activation) and enhancement of chemoreceptors. The ergoreflexes, a neurally mediated reflex arising from exercising muscle in proportion to work done, is enhanced.

All rights reserved. No part of this programme may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without the prior permission of the publishers, Medinews (Cardiology) Limited.
It shall not, by way of trade or otherwise, be lent, re-sold, hired or otherwise circulated without the publisher’s prior consent.
Medical knowledge is constantly changing. As new information becomes available, changes in treatment, procedures, equipment and the use of drugs becomes necessary. The editors/authors/contributors and the publishers have taken care to ensure that the information given in this text is accurate and up to date. Readers are strongly advised to confirm that the information, especially with regard to drug usage, complies with the latest legislation and standards of practice.
Healthcare professionals should consult up-to-date Prescribing Information and the full Summary of Product Characteristics available from the manufacturers before prescribing any product. Medinews (Cardiology) Limited cannot accept responsibility for any errors in prescribing which may occur.