Presentation and outcomes of patients with ST-elevation myocardial infarction (STEMI) may change during viral pandemics. We compared symptom-to-call (STC), call-to-balloon (CTB), door-to-balloon (DTB) times; high-sensitivity troponin (hs-cTnI) levels; and survival of patients (n=39) during the first wave of the COVID-19 pandemic (defined as a ‘COVID period’ starting four weeks before lockdown) to historical controls from a ‘pre-COVID period’ (n=45).
STEMI admissions fell one week before lockdown by 29%. Median STC times began to rise one month before lockdown (54 vs. 25 min, p=0.06), with peak increases between 9 March and 5 April (166 vs. 59 min, p=0.04). Median CTB and DTB times were unchanged. Mean peak hs-cTnI increased during COVID-19 (15,225 vs. 8,852 ng/ml, p=0.004). Six-month survival following all STEMI reduced (82.1% vs. 95.6%, p<0.05).
STC times are the earliest indicator that STEMI-patient behaviour changed four weeks before lockdown, correlating with higher troponin levels and reduced survival. These early signals could guide public health interventions during future pandemics.
Introduction
Delays in treatment following ST-elevation myocardial infarction (STEMI) influence patient outcomes. During the first wave of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2, COVID-19) pandemic, delays in treatment may have altered outcomes of STEMI patients, even in those not infected by COVID-19.
On 11 March 2020, the World Health Organisation declared COVID-19 a global pandemic.1 The UK government mandated social distancing on 16 March 2020, and imposed a nationwide lockdown on 23 March 2020.2 Primary percutaneous coronary intervention (PCI) remained our centre’s treatment of choice for STEMI, with thrombolysis reserved for patients with suspected COVID-19 unable to lie flat despite non-invasive ventilation (NIV).
National data show a reduction in primary PCI procedures for STEMI during lockdown.3-5 The effect of COVID-19 on symptom-to-call (STC), call-to-balloon (CTB) and door-to-balloon (DTB) times has varied. The temporal relationship between lockdown, presentation times and admission numbers, and the effects on mortality following STEMI are unclear.5,6 As far as we know, there are no published data on six-month outcomes.
We performed a retrospective analysis of STEMI patients at a single UK primary PCI centre, studying the effect of COVID-19 on STEMI admissions, treatment, presentation times, times to revascularisation, increases in high-sensitivity troponin (hs-cTnI), left ventricular ejection fraction (LVEF), 30-day and six-month mortality.
Method
Data collection
We analysed data on STEMI patients at Frimley Park Hospital, Surrey, UK, using hospital records, local Myocardial Ischaemia National Audit Project (MINAP) and British Cardiovascular Interventional Society (BCIS) databases. Frimley Park Hospital treats STEMI patients from Surrey, Berkshire and Hampshire, covering a catchment area of one million patients and performing between 250 and 350 primary PCIs per year. Electrocardiograms (ECGs) are transmitted from ambulances to the coronary care unit to keep inappropriate activations to a minimum. Our analysis included all STEMI patients, regardless of whether they received primary PCI or not.
A preliminary analysis identified an increase in STC times from 23 February 2020. We, therefore, defined a ‘COVID period’ between 23 February and 28 April 2020, four weeks prior to, and 5 weeks post, the introduction of the national lockdown. A historical control group – ‘pre-COVID period’ – was defined between 23 February and 28 April 2019, one year prior to the pandemic.
We analysed demographics and presentation characteristics (table 1); procedural characteristics (vascular access site, use of thrombus aspiration or glycoprotein IIb/IIIa antagonists); STC, CTB and DTB times; hs-cTnI levels (via Siemens ADVIA Centaur® XP immunoassay system); LVEF up to four weeks post-STEMI; in-hospital, 30-day and three-month mortality, and six-month survival.
Table 1. Interventions for patients after first event
| Baseline demographics | COVID period, % (95%CI) | Pre-COVID period, % (95%CI) | Chi-squared statistic | p value |
|---|---|---|---|---|
| Male | 75.6 (61.2 to 85.9) | 61.5 (45.9 to 75.1) | 1.9208 | 0.17 |
| Previous MI | 11.1 (4.4 to 24.0) | 12.8 (5.1 to 27.2) | 0.0582 | 0.81 |
| Previous angina | 17.8 (9.0 to 31.6) | 17.9 (8.7 to 33) | 0.0004 | 0.98 |
| Hypertension | 42.2 (30.0 to 56.7) | 35.9 (22.7 to 51.6) | 0.3594 | 0.55 |
| Hypercholesterolaemia | 33.3 (21.3 to 48.0) | 23.1 (12.4 to 38.5) | 1.0769 | 0.30 |
| PVD | 11.1 (4.4 to 24.0) | 2.6 (<0.01 to 14.4) | 2.3011 | 0.13 |
| CVD | 0 | 2.6 (<0.01 to 14.4) | 0.4643 | >0.05† |
| Diabetes (type 1 or 2) | 11.1 (4.4 to 24.0) | 15.4 (6.9 to 30.1) | 0.3353 | 0.56 |
| Asthma/COPD | 8.9 (3.0 to 21.3) | 5.1 (0.5 to 17.8) | 0.4455 | 0.50 |
| CRF | 0 | 2.6 (<0.01 to 14.4) | 0.4643 | >0.05† |
| Heart failure | 0 | 2.6 (<0.01 to 14.4) | 0.4643 | >0.05† |
| Current smokers | 22.2 (12.4 to 36.5) | 33.3 (20.6 to 49.1) | 1.9145 | 0.17 |
| 0.17 | ||||
| Direct admissions to catheter lab | 64.4 (49.8 to 76.8) | 74.4 (58.8 to 85.6) | 0.9609 | 0.32 |
| Self-presenters | 15.6 (7.4 to 29.1) | 15.4 (6.9 to 30.1) | 0.0005 | 0.98 |
| Inter-hospital transfer | 15.6 (7.4 to 29.1) | 7.7 (1.9 to 21.0) | 1.2318 | 0.27 |
| Prior on DAPT | 20.0 (10.7 to 34.0) | 12.8 (5.1 to 27.2) | 0.7754 | 0.38 |
| DAPT started following STEMI | 77.8 (63.6 to 87.6) | 87.2 (72.8 to 94.9) | 0.8593 | 0.35 |
| STEMI territory | ||||
| Anterior MI | 51.1 (37.0 to 65.0) | 53.8 (38.6 to 68.4) | 0.0627 | 0.80 |
| Inferior MI | 37.8 (25.1 to 52.4) | 38.5 (24.9 to 54.1) | 0.0041 | 0.95 |
| Posterior/lateral MI | 11.1 (4.4 to 24.0) | 7.7 (1.9 to 21.0) | 0.2834 | 0.59 |
| †Fisher’s exact method used to calculate significance. Key: CI = confidence interval; COPD = chronic obstructive pulmonary disease; CRF = chronic renal failure; CVA = cerebrovascular accident; CVD = cardiovascular disease; DAPT = dual antiplatelet therapy; MI = myocardial infarction; PVD = peripheral vascular disease; STEMI = ST-elevation myocardial infarction |
||||
Statistical analysis
Quantitative comparisons included Pearson’s Chi-square or Fisher’s exact test (categorical variables) and Z-tests (proportions in continuous data). Continuous data were compared using the two-tailed Mann-Whitney U test (medians) or Student’s t-test (means); 95% confidence intervals (CIs) calculated using the Adjusted Wald Method (proportions) and t-distribution method (continuous data). Pearson’s Chi-square test compared mortality and the log-rank test calculated six-month survival probability. Statistical significance was assessed to 0.05 level. Data were analysed using Microsoft Excel with the Analysis ToolPak add-in.
Results
Of 39 STEMI patients in the COVID period, one presented with COVID-19 symptoms, was unable to lie flat despite NIV and was thrombolysed; 38.5% received a coronavirus RNA swab (before swabbing of all patients became mandatory), all of which were negative. The pre-COVID period contained 45 STEMI patients.
Baseline demographics and presentation characteristics
Mean age in the COVID and pre-COVID periods was 62.8 (95%CI 58.3 to 67.4) years and 66.2 (95%CI 63.3 to 69.2) years, respectively (p=0.23). There were no differences in the baseline demographic characteristics, route of admission or territory of infarction (table 1).
STEMI admissions
There was an overall 13% reduction in STEMI admissions during the COVID period, from 45 to 39 (incidence rate ratio [IRR] 0.87, 95%CI 0.56 to 1.33, p=0.05) with admissions falling from 16 March 2020 (figure 1). Between 16 March and 28 April 2020 admissions reduced 29% compared with equivalent dates in 2019, from 31 to 22 (IRR 0.71, 95%CI 0.41 to 1.23, p=0.05).

Upper axis: Mean symptom-to-call (STC) times for each two-weekly interval in the four weeks preceding and succeeding national lockdown on 23 March 2020 (COVID period, red line) versus equivalent 2019 periods (pre-COVID period, blue line)
Proportion of primary PCI performed for STEMI admissions
Of 39 patients in the COVID period, 29 activated the primary PCI pathway and underwent angiography, of which 27 underwent primary PCI (69.2% of the initial cohort, 95%CI 53.5 to 81.5%). Of 45 patients in the pre-COVID period, 41 activated the primary PCI pathway and underwent angiography, of which 40 underwent primary PCI (88.9%, 95%CI 76.1 to 95.6%, p=0.03). There were no inappropriate activations.
STC time
A preliminary analysis showed median STC times began to increase four weeks before lockdown, with an overall median time of 54 minutes (interquartile ratio [IQR] 149) during the COVID period versus 26 minutes during the pre-COVID period (IQR 102) (p=0.06). Mean STC time differences peaked between 9 March and 5 April (166 vs. 59 minutes, p=0.04) (figure 1). After 6 April, these differences appeared to resolve.
CTB time and DTB time
The COVID and pre-COVID periods had 22 and 27 STEMIs respectively with recorded CTB times (excludes self-presenters). Median times were similar, 103 minutes (IQR 54) and 99 minutes (IQR 48), respectively (p=0.33). Median DTB time in the COVID (n=27) and pre-COVID (n=39) periods were not significantly different, 34 minutes (IQR 77) versus 37 minutes (IQR 32) (p=0.93).
Angiographic and procedural characteristics
Use of glycoprotein IIb/IIIa antagonists did not differ, 58.6% (95%CI 40.7 to 74.5%) versus 55.0% (95%CI 39.8 to 69.3%) (p=0.77). Radial arterial access was higher in the COVID period, 96.6% (95%CI 81.4 to >99.9%) versus 82.1% (95%CI 67.0 to 91.3%) (p=0.07). In the pre-COVID period, five of eight cases using femoral access were post-cardiac arrest or cardiogenic shock. There was a significant increase in use of thrombus aspiration in the COVID period, 44.8% (95%CI 28.4 to 62.5%) versus 10.0% (95%CI 3.4 to 23.6%) (p<0.001).
Troponin rise
Mean hs-cTnI rise significantly increased in the COVID period, 15,225 (95%CI 11,924 to 18,523) versus 8,852 (95%CI 6,295 to 11,410) ng/ml (p=0.004), as did the proportion of patients with hs-cTnI >25,000 ng/ml, 48.7% (95%CI 33.9 to 63.8%) versus 13.3% (95%CI 5.9 to 26.6%) (p<0.001).
Ejection fraction
Echocardiograms up to four weeks post-STEMI in 32 COVID period and 41 pre-COVID period patients demonstrated no difference in mean LVEF, 43.7% versus 41.8%, respectively (p=0.47).
Mortality
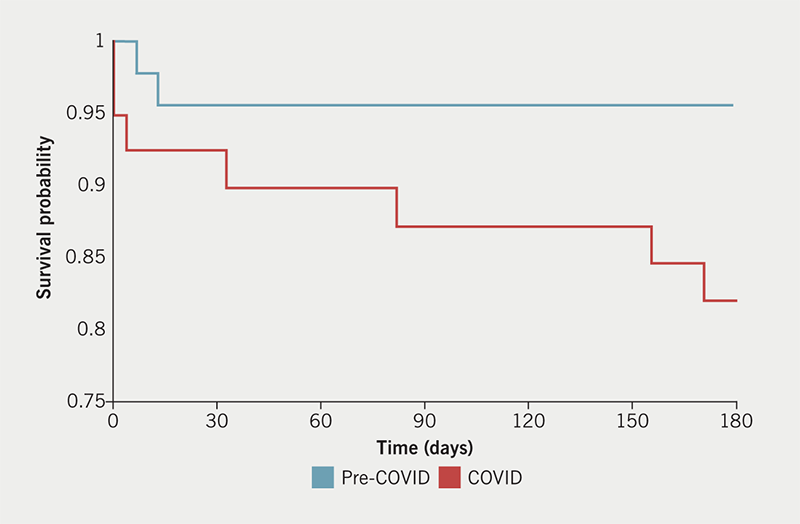
Mortality of all STEMI patients was not significantly different between the COVID and pre-COVID periods in-hospital (7.7 vs. 2.2%, p=0.24), at 30 days (7.7 vs. 4.4%, p=0.53) and three months (12.8 vs. 4.4%, p=0.17). However, six-month survival of all STEMI patients during the COVID period significantly reduced (82.1 vs. 95.6%, p<0.05) (figure 2). Where patients received primary PCI, six-month survival was similar (97.8 vs. 97.4%, p=0.93).
Discussion
We examined the impact of the first COVID-19 pandemic wave on STEMI patients at a single UK primary PCI centre. STC times, a surrogate marker for patient behaviour, began to rise one month prior to the national lockdown (23 March 2020) and three weeks before the social distancing mandate (16 March 2020). Overall, median STC times rose by 108% compared with a 2019 ‘pre-COVID’ control period. STC time differences peaked between 9 March and 5 April 2020 (166 vs. 59 minutes). Other studies have also described increased symptom-to-first-medical-contact times during the pandemic.4,7-9 Three weeks after STC times began to rise, and one week before national lockdown, we observed a fall in STEMI admissions and a 29% reduction in STEMI admissions between 16 March and 28 April 2020. UK and international studies have described similar changes,8,10-12 but to our knowledge, the temporal relationship between these changes has not been described elsewhere.
We identify increasing STC times as the earliest signal of changing STEMI patient behaviour during a viral pandemic. Health messages such as ‘stay at home, save the NHS’ and the fear of contracting COVID-19 from health services13 may have contributed to this effect. STC times normalised after 6 April 2020. We recommend that future public health messaging may be sensitive to these signals of patient behaviour.
The proportion of catheter lab activations following STEMI reduced from 93.3% (95%CI 81.5 to 98.3%) to 74.4% (95%CI 58.8 to 85.6%). Reductions in primary PCI activations for STEMI up to 43% have been described elsewhere.3-5 Our CTB (103 vs. 99 minutes) and DTB times (34 vs. 39 minutes) were unaffected despite changes to the STEMI-management protocols during the pandemic. Other studies have shown no change in CTB (110 vs. 110 minutes)7 or DTB times,14 but also increased DTB times (83.3 vs. 61 and 110 vs. 84.5 minutes).4,9 Our data support maintaining primary PCI as the gold-standard STEMI treatment over thrombolysis during this pandemic.
The use of mechanical thrombus aspiration increased in the COVID period, 44.8% (95%CI 28.4 to 62.5%) versus 10.0% (95%CI 3.4 to 23.6%). Similar increases have been observed in STEMI patients with concurrent COVID-19 infection (17.9% vs. 1.3%).15 Prolonged STC times and/or abnormal coagulation associated with undiagnosed COVID-19 infection may explain our observation.16
Mean peak hs-cTnI rise was significantly higher in the COVID period (15,225 vs. 8,852 ng/ml). Patients with peak troponin rises <5,000 ng/ml significantly reduced (25.6% vs. 48.9%), while those with rises >25,000 ng/ml increased (48.7% vs. 13.3%). Peak cardiac troponin rise correlates with crude infarct size,17 but we saw no difference in LVEF four weeks post-STEMI between both periods.
In-hospital and 30-day mortality following STEMI tended to be higher but did not reach significance during the COVID period (7.7 vs. 2.2% and 7.7 vs. 4.4%, respectively). Other UK studies have reported no change,5 increased mortality,7,18 and a fall in 30-day mortality from 10.2% to 7.7%.6 We show for the first time that six-month survival in all STEMI patients during the COVID period significantly reduced from 95.6% to 82.1%. Factors influencing reduced survival may include prolonged STC times and fewer catheter lab activations. In those STEMI patients treated by primary PCI, there was no difference in six-month survival (97.8% vs. 97.4%).
In summary, we observed a rise in STC times one month prior to national lockdown and three weeks before STEMI admissions began to fall during the first wave of the COVID-19 pandemic. This may represent the earliest documented signal of changing STEMI-patient behaviour during a viral pandemic. These signals may be exploited to trigger earlier public health interventions in future pandemics. We also observed a possible correlation between prolonged STC times, reduced STEMI admissions, greater use of thrombus aspiration during primary PCI, higher peak hs-cTnI levels and reduced six-month survival following STEMI.
Our study has many limitations. Small sample sizes mean many perceived differences may have happened by chance or influenced outcome data. Only a small proportion of COVID period patients were swabbed. Cases labelled as COVID myocarditis may not have entered the MINAP database and so may have been missed. A single-centre retrospective observational study may be influenced by local population and service factors. Nevertheless, this provides valuable data on the impact of the COVID-19 pandemic on STEMI patients at a single UK primary PCI centre and suggests that STC times might be a useful marker for early changes in cardiac-patient behaviour. Hypotheses generated by our study could be tested with larger datasets in future studies.
Key messages
- During the first COVID-19 pandemic wave, we observed rising symptom-to-call (STC) times three weeks before ST-elevation myocardial infarction (STEMI) admissions began to fall, and four weeks before national lockdown
- Increased STC times correlated with increased peak high-sensitivity cardiac troponin levels, and reduced six-month survival following all STEMI during the pandemic
- Rising STC times may be a surrogate marker for changing patient behaviour during pandemics prior to national lockdowns, and correlate with poor clinical outcomes. This marker could be used as an early warning signal to trigger earlier public health interventions
Conflicts of interest
None declared.
Funding
None.
Study approval
This service evaluation was registered with the clinical audit department and followed local and national audit and ethics guidelines. Data were acquired from anonymised national databases of non-identifiable patient data.
Acknowledgements
With thanks to Adam Fox for help with data collection and all members of the Frimley Park Hospital primary PCI service.
References
1. World Health Organization. WHO Director-General’s opening remarks at the media briefing on COVID-19. 11 March 2020. Available at: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19—11-march-2020
2. Gov.uk. Prime Minister’s statement on coronavirus (COVID-19): 23 March 2020. Available at: https://www.gov.uk/government/speeches/pm-address-to-the-nation-on-coronavirus-23-march-2020
3. Rodríguez-Leor O, Cid-Álvarez B, Ojeda S et al. Impact of the COVID-19 pandemic on interventional cardiology activity in Spain. REC Interv Cardiol 2020;2:82–9. https://doi.org/10.24875/RECICE.M20000123
4. Tam CF, Cheung KS, Lam S et al. Impact of coronavirus disease 2019 (COVID-19) outbreak on ST-segment-elevation myocardial infarction care in Hong Kong, China. Circ Cardiovasc Qual Outcomes 2020;13:e006631. https://doi.org/10.1161/CIRCOUTCOMES.120.006631
5. Kwok CS, Gale CP, Kinnaird T et al. Impact of COVID-19 on percutaneous coronary intervention for ST-elevation myocardial infarction. Heart 2020;106:1805–11. https://doi.org/10.1136/heartjnl-2020-317650
6. Wu J, Mamas M, Rashid M et al. Patient response, treatments, and mortality for acute myocardial infarction during the COVID-19 pandemic. Eur Heart J Qual Care Clin Outcomes 2020;7:238–46. https://doi.org/10.1093/ehjqcco/qcaa062
7. Rodríguez-Leor O, Cid-Álvarez B, Pérez de Prado A et al. Impact of COVID-19 on ST-segment elevation myocardial infarction care. The Spanish experience. Rev Esp Cardiol (Engl Ed) 2020;73:994–1002. https://doi.org/10.1016/j.rec.2020.08.002
8. Abdelaziz HK, Abdelrahman A, Nabi A et al. Impact of COVID-19 pandemic on patients with ST-segment elevation myocardial infarction: insights from a British cardiac center. Am Heart J 2020;226:45–8. https://doi.org/10.1016/j.ahj.2020.04.022
9. Fu X-Y, Shen X-F, Cheng Y-R et al. Effect of COVID-19 outbreak on the treatment time of patients with acute ST-segment elevation myocardial infarction. Am J Emerg Med 2021;44:192–7. https://doi.org/10.1016/j.ajem.2020.09.038
10. Mesnier J, Cottin Y, Coste P et al. Hospital admissions for acute myocardial infarction before and after lockdown according to regional prevalence of COVID-19 and patient profile in France: a registry study. Lancet Public Health 2020;5:e536–e542. https://doi.org/10.1016/S2468-2667(20)30188-2
11. National Institute for Cardiovascular Outcomes Research (NICOR). NICOR COVID-19 report. London: NICOR. Available from: https://www.nicor.org.uk/covid-19-and-nicor/nicor-covid-19-report/
12. Mafham MM, Spata E, Goldacre R et al. COVID-19 pandemic and admission rates for and management of acute coronary syndromes in England. Lancet 2020;396:381–9. https://doi.org/10.1016/S0140-6736(20)31356-8
13. Patel S, Lorenzi N, Smith T, Carlson BR, Sternberg P. Critical insights from patients during the Covid-19 pandemic. NEJM Catal Innov Care Deliv 2020; published online 13 July 2020. https://doi.org/10.1056/CAT.20.0299
14. Tan W, Parikh RV, Chester R et al. Single center trends in acute coronary syndrome volume and outcomes during the COVID-19 pandemic. Cardiol Res 2020;11:256–9. https://doi.org/10.14740/cr1096
15. Choudry FA, Hamshere SM, Rathod KS et al. High thrombus burden in patients with COVID-19 presenting with ST-segment elevation myocardial infarction. J Am Coll Cardiol 2020;76:1168–76. https://doi.org/10.1016/j.jacc.2020.07.022
16. Abou-Ismail MY, Diamond A, Kapoor S, Arafah Y, Nayak L. The hypercoagulable state in COVID-19: incidence, pathophysiology, and management. Thromb Res 2020;194:101–15. https://doi.org/10.1016/j.thromres.2020.06.029
17. Chia S, Senatore F, Raffel OC, Lee H, Wackers FJ, Jang IK. Utility of cardiac biomarkers in predicting infarct size, left ventricular function, and clinical outcome after primary percutaneous coronary intervention for ST-segment elevation myocardial infarction. JACC Cardiovasc Interv 2008;1:415–23. https://doi.org/10.1016/j.jcin.2008.04.010
18. Chen Y, Rathod KS, Hamshere S et al. COVID-19 and changes in activity and treatment of ST elevation MI from a UK cardiac centre. Int J Cardiol Heart Vasc 2021;33:100736. https://doi.org/10.1016/j.ijcha.2021.100736
