Introduction
Effective management of cardiovascular risk factors following acute coronary syndrome (ACS) is crucial for reducing the risk of recurrent cardiovascular events and improving long-term patient outcomes. Adherence to evidence-based therapies and lifestyle modifications can significantly lower the incidence of adverse events, including recurrent ACS, stroke, and heart failure, while also improving quality of life for patients after ACS. Continuously monitoring and adjusting treatment strategies based on individual patient risk profiles is vital for optimising outcomes and reducing the burden of cardiovascular disease.
This module reviews the management options that should be considered post-ACS for each patient, including both pharmacological treatment and behavioural interventions.
Post-ACS antithrombotic therapy
Dual antiplatelet therapy (DAPT), consisting of aspirin and a P2Y12 inhibitor (clopidogrel, ticagrelor, or prasugrel), remains the cornerstone of post-ACS antithrombotic therapy. The 2023 European Society of Cardiology (ESC) guidelines for the management of acute coronary syndromes emphasise the importance of DAPT in reducing recurrent ischaemic events following ACS.1
Among the P2Y12 inhibitors, ticagrelor and prasugrel are preferred over clopidogrel in most ACS patients due to their superior efficacy in preventing ischaemic events, including myocardial infarction and stent thrombosis.2,3
The standard duration for DAPT post-ACS is 12 months, as this period effectively reduces the risk of recurrent ischaemic events, including stent thrombosis and ACS. However, the duration of DAPT may be adjusted based on individual patient risk factors such as bleeding risk and risk of recurrent ischaemic events (figure 1 and table 1).4,5
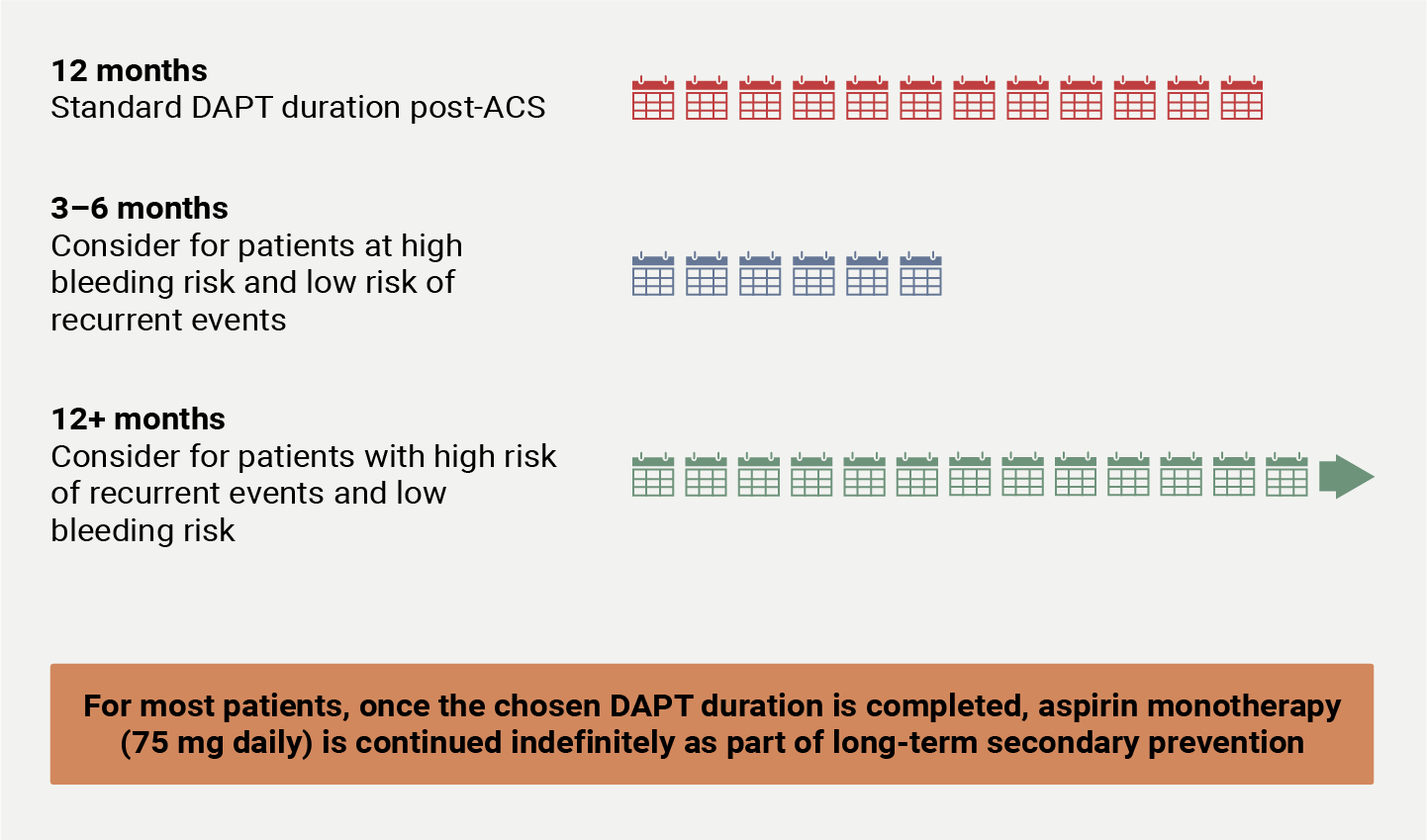
Table 1. Bleeding and ischaemic risk determinants
style=”background-color: lightgrey; border-bottom: 2px solid grey; padding: 5px;
| Risk factor | Bleeding risk | Ischaemic risk |
| Age | ↑ with age >75 years | ↑ with comorbidities |
| Body weight | ↑ if weight <60 kg | ↑ in morbid obesity and malnourished states |
| Renal function | ↑ with eGFR <30 mL/min/1.73 m2 | ↑ in renal impairment, especially with CAD |
| History of major bleeding | ↑↑ bleeding risk | ↔ effect, but may impact DAPT duration |
| Diabetes mellitus | ↔ effect | ↑ due to thrombosis and endothelial dysfunction |
| CAD | ↔ effect | ↑ especially with multi-vessel disease and prior ACS |
| Stent type and complexity | ↑ with drug-eluting stents | ↑ with complex or multi-vessel coronary disease |
| Concurrent anticoagulation | ↑ with oral anticoagulants | ↔ effect, but relevant in treatment strategy |
| History of stroke | ↑ especially with history of intracranial bleeding | ↑ especially with other peripheral arterial disease |
| Gastrointestinal conditions | ↑ with GI disorders or peptic ulcers | ↔ effect |
| Current or previous cancer | ↑ with active cancer and treatments | ↔ effect |
| Thrombophilia | ↔ effect | ↑ due to increased thrombotic tendency |
| Platelet count/function | ↑ with low platelet count or dysfunction | ↑ with platelet dysfunction due to impaired thrombus formation |
| Key: ↑ = increased risk; ↔ no significant effect; ↓ decreased risk; ACS = acute coronary syndrome; CAD = coronary artery disease; DAPT = dual antiplatelet therapy; GI = gastrointestinal | ||
In individuals at higher risk of an ischaemic stroke, aspirin and low-dose rivaroxaban was the most effective in reducing stroke should a strategy for prolonged, intensified antithrombotic therapy be chosen.6
Finally, the 2023 ESC Guidelines1 recommend that in patients with an indication for oral anticoagulation therapy, DAPT is added for a short period of up to one month, followed by de-escalation to OAC and clopidogrel for a further 11 months, before returning to OAC monotherapy.
Lipid management
Aggressive lipid-lowering therapy is pivotal in secondary prevention post-ACS. Lipid management is discussed in greater detail in module 3.
Step 1: Statin therapy
The 2023 ESC Guidelines1 recommend high-intensity statins to achieve a low-density lipoprotein cholesterol (LDL-C) target of <55 mg/dL (1.4 mmol/L) or a reduction of ≥50% from baseline levels. For very high-risk patients, an LDL-C target of <40 mg/dL (1.0 mmol/L) is advised.
Statins have a robust body of evidence supporting their efficacy in reducing major cardiovascular events and mortality post-ACS.7 Additionally, combination therapy with statins and ezetimibe has been shown to provide enhanced protection against recurrent cardiovascular events.8
Step 2: Ezetimibe
If LDL levels remain above target despite maximally tolerated statin therapy, the addition of ezetimibe is recommended.
Step 3: PCSK9 inhibition
Should further reduction be necessary, proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors (e.g., evolocumab, alirocumab) are recommended.9,10
Additional therapy at any step: Icosapent ethyl
In high-risk patients with persistently high triglycerides (≥135 mg/dL or ≥1.5 mmol/L) despite statin therapy, icosapent ethyl (2 g twice daily) may be considered to further reduce cardiovascular risk. This therapy is particularly beneficial in patients who remain at high risk despite optimised statin therapy.11
Blood pressure and glycaemic control
Blood pressure
Effective blood pressure (BP) management is crucial post-ACS. The 2023 ESC Guidelines recommend a target BP of <130/80 mmHg.1 See table 2 for the recommended medication classes for blood pressure control in ACS.
Table 2: Medication classes recommended for blood pressure control post-acute coronary syndrome (ACS)1
style=”background-color: lightgrey; border-bottom: 2px solid grey; padding: 5px;
| Angiotensin-converting enzyme inhibitors (ACEIs) or angiotensin receptor blockers (ARBs) | Beta blockers | Mineralocorticoid receptor antagonists (MRAs) |
First-line agents – particularly in patients with:
|
Advised for all patients post-ACS, particularly those with left ventricular ejection fraction ≤40%, as they have been shown to improve survival | Recommended post-ACS for patients with left ventricular dysfunction and heart failure or diabetes, to reduce morbidity and mortality |
Diabetes management
Diabetes significantly increases cardiovascular risk post-ACS. The 2023 ESC Guidelines1 advocate for optimal glycaemic control with a glycated haemoglobin A1c (HbA1c) target of <7% (53 mmol/mol).1
Beyond metformin, sodium-glucose cotransporter-2 (SGLT2) inhibitors (e.g., empagliflozin, dapagliflozin) and glucagon-like peptide-1 receptor agonists (GLP-1 RAs) (e.g., liraglutide, semaglutide) are recommended due to their proven cardiovascular benefits. These therapies have proven to have pleiotropic effects, improving both glycaemic control and cardiovascular outcomes post-ACS.
Table 3. Medication classes for patients with diabetes mellitus post-acute coronary syndrome (ACS)1
style=”background-color: lightgrey; border-bottom: 2px solid grey; padding: 5px;
| Sodium–glucose cotransporter-2 (SGLT2) inhibitors | Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) |
| Shown to reduce heart failure hospitalisations and cardiovascular mortality1 | Demonstrated reductions in major adverse cardiovascular events12 |
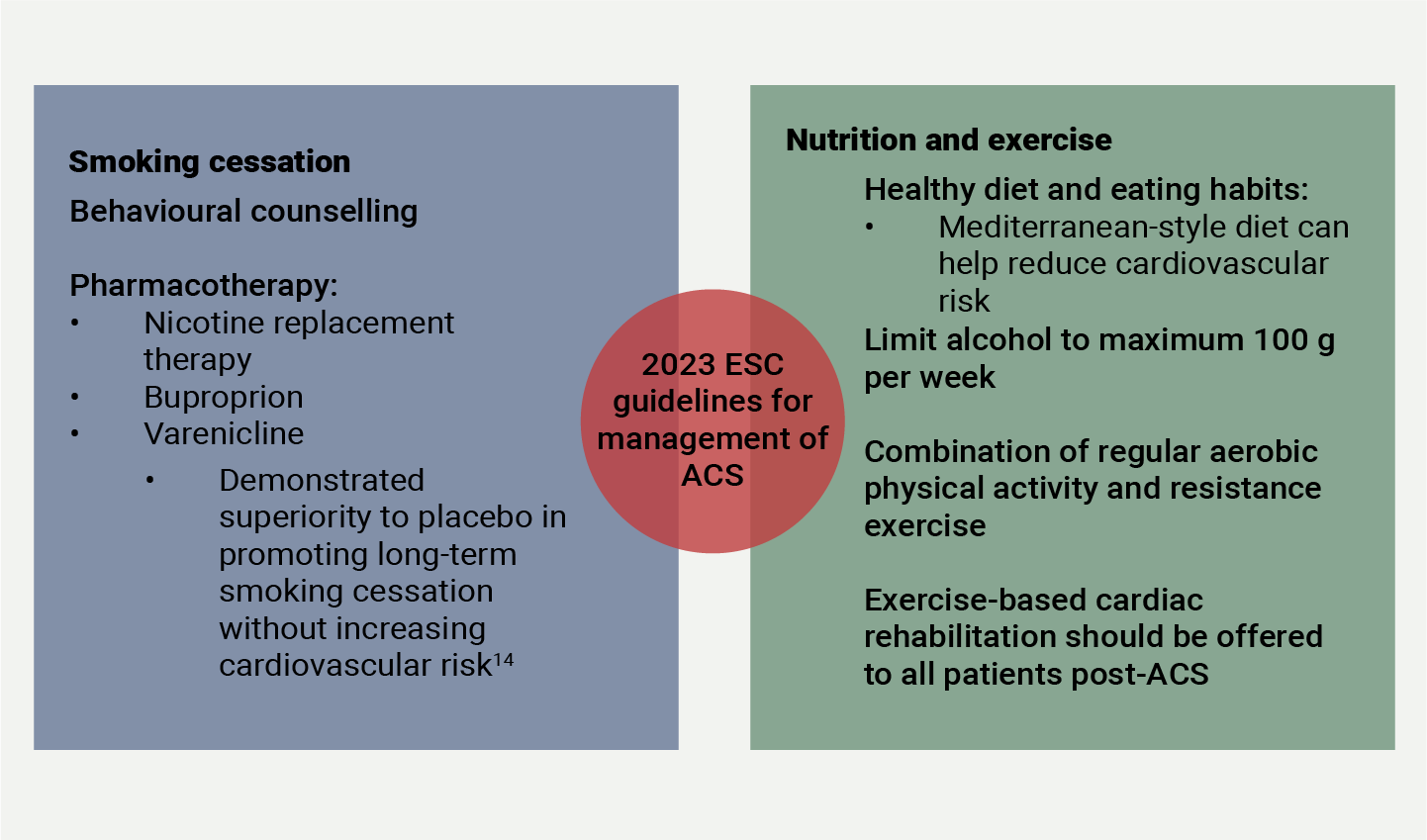
Lifestyle and behavioural interventions
Lifestyle and behavioural interventions recommended post-ACS are summarised in figure 2.
| Key: ESC = The European Society of Cardiology |
Smoking cessation
Smoking remains a major modifiable risk factor for recurrent cardiovascular events post-ACS.13,14 The 2023 ESC Guidelines strongly recommend smoking cessation interventions to improve quit rates and reduce cardiovascular risks.1
Weight management and diet
Obesity and poor dietary habits are significant risk factors for adverse cardiovascular outcomes post-ACS. The 2023 ESC Guidelines recommend sustained weight loss to improve metabolic parameters and cardiovascular health, with a focus on gradual weight reduction through a combination of dietary modifications and physical activity.1
Adherence to a Mediterranean diet, which is rich in vegetables, fruits, whole grains, fish, and olive oil, is advised to reduce major cardiovascular events. The Mediterranean diet has been shown to lower the incidence of cardiovascular events and improve long-term survival after myocardial infarction.15 A reduction in daily sodium intake by 2.5 g reduced adverse cardiovascular outcomes.16
Additionally, in patients with severe obesity (BMI ≥40 kg/m2 or ≥35 kg/m2 with comorbidities), bariatric surgery may be considered to improve cardiovascular outcomes and reduce long-term cardiovascular mortality.17
Key messages
- Antithrombotic therapy must be optimised in the post-ACS setting. Dual antiplatelet therapy (DAPT) with aspirin and a P2Y12 inhibitor (preferably ticagrelor or prasugrel) remains the cornerstone of post-ACS management, with treatment duration tailored to ischaemic and bleeding risks. Long-term aspirin monotherapy is recommended for most patients. For patients with an indication for oral anticoagulation therapy, DAPT with aspirin and clopidogrel is added for a short period of up to one month, followed by de-escalation to OAC and clopidogrel for a further 11 months, before returning to OAC monotherapy.
- Comprehensive risk factor management can reduce the risk of secondary events. Secondary prevention strategies include aggressive lipid-lowering therapy, tight blood pressure control (<130/80 mmHg), and diabetes management with SGLT2 inhibitors or GLP-1 RAs for added cardiovascular benefits.
- Lifestyle and behavioural interventions should not be neglected. Smoking cessation, weight management, and adherence to a Mediterranean diet are strongly recommended to reduce recurrent cardiovascular events. Pharmacologic and surgical options (e.g., bariatric surgery) may be considered for high-risk patients with obesity.
References
1. Byrne RA, Rossello X, Coughlan JJ et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart J 2023;44:3720–826. https://doi.org/10.1093/eurheartj/ehad191
2. Wallentin L, Becker RC, Budaj A et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N Engl J Med 2009;361:1045–57. https://doi.org/10.1056/nejmoa0904327
3. Wiviott SD, Braunwald E, McCabe CH et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N Engl J Med 2007;357:2001–15. https://doi.org/10.1056/nejmoa0706482
4. Capodanno D, Laudani C. Unraveling the maze of de-escalation strategies in acute coronary syndromes. Circ Cardiovasc Interv 2023;16:e013461. https://doi.org/10.1161/circinterventions.123.013461
5. Valgimigli M, Landi A, Angiolillo DJ et al. Demystifying the contemporary role of 12-month dual antiplatelet therapy after acute coronary syndrome. Circulation 2024;150:317–35. https://doi.org/10.1161/circulationaha.124.069012
6. Navarese EP, Landi A, Oliva A et al. Within and beyond 12-month efficacy and safety of antithrombotic strategies in patients with established coronary artery disease: two companion network meta-analyses of the 2022 joint clinical consensus statement of the European Association of Percutaneous Cardiovascular Interventions (EAPCI), European Association for Acute CardioVascular Care (ACVC), and European Association of Preventive Cardiology (EAPC). Eur Heart J Cardiovasc Pharmacother 2023;9:271–90. https://doi.org/10.1093/ehjcvp/pvad016
7. Navarese EP, Kowalewski M, Andreotti F et al. Meta-analysis of time-related benefits of statin therapy in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Am J Cardiol 2014;113:1753–64. https://doi.org/10.1016/j.amjcard.2014.02.034
8. Cannon CP, Blazing MA, Giugliano RP et al. Ezetimibe added to statin therapy after acute coronary syndromes. N Engl J Med 2015;372:2387–97. https://doi.org/10.1056/nejmoa1410489
9. Sabatine MS, Giugliano RP, Keech AC et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med 2017;376:1713–22. https://doi.org/10.1056/nejmoa1615664
10. Schwartz GG, Steg PG, Szarek M et al. Alirocumab and cardiovascular outcomes after acute coronary syndrome. N Engl J Med 2018;379:2097–107. https://doi.org/10.1056/nejmoa1801174
11. Bhatt DL, Steg PG, Miller M et al. Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia. N Engl J Med 2019;380:11–22. https://doi.org/10.1056/nejmoa1812792
12. Kristensen SL, Rørth R, Jhund PS et al. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet Diabetes Endocrinol 2019;7:776–85. https://doi.org/10.1016/s2213-8587(19)30249-9
13. Chow CK, Jolly S, Rao-Melacini P et al. Association of diet, exercise, and smoking modification with risk of early cardiovascular events after acute coronary syndromes. Circulation 2010;121:750–8. https://doi.org/10.1161/circulationaha.109.891523
14. Windle SB, Dehghani P, Roy N et al. Smoking abstinence 1 year after acute coronary syndrome: follow-up from a randomized controlled trial of varenicline in patients admitted to hospital. Cmaj 2018;190:E347–54. https://doi.org/10.1503/cmaj.170377
15. Estruch R, Ros E, Salas-Salvadó J, Covas MI, Corella D, Arós F et al. Primary prevention of cardiovascular disease with a Mediterranean diet supplemented with extra-virgin olive oil or nuts. N Engl J Med 2018;378:e34. https://doi.org/10.1056/nejmoa1800389
16. He FJ, Tan M, Ma Y, MacGregor GA. Salt reduction to prevent hypertension and cardiovascular disease: JACC state-of-the-art review. J Am Coll Cardiol 2020;75:632–47. https://doi.org/10.1016/j.jacc.2019.11.055
17. Cardoso L, Rodrigues D, Gomes L, Carrilho F. Short- and long-term mortality after bariatric surgery: a systematic review and meta-analysis. Diabetes Obes Metab 2017;19:1223–32. https://doi.org/10.1111/dom.12922

All rights reserved. No part of this programme may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without the prior permission of the publishers, Medinews (Cardiology) Limited.
It shall not, by way of trade or otherwise, be lent, re-sold, hired or otherwise circulated without the publisher’s prior consent.
Medical knowledge is constantly changing. As new information becomes available, changes in treatment, procedures, equipment and the use of drugs becomes necessary. The editors/authors/contributors and the publishers have taken care to ensure that the information given in this text is accurate and up to date. Readers are strongly advised to confirm that the information, especially with regard to drug usage, complies with the latest legislation and standards of practice.
Healthcare professionals should consult up-to-date Prescribing Information and the full Summary of Product Characteristics available from the manufacturers before prescribing any product. Medinews (Cardiology) Limited cannot accept responsibility for any errors in prescribing which may occur.