Cardiovascular disease is a leading cause of mortality in patients with chronic kidney disease (CKD) and kidney transplant recipients (KTR). However, it remains uncertain whether KTR status predisposes patients to a heightened risk of major adverse cardiovascular events (MACE) following percutaneous coronary intervention (PCI). A systematic search was conducted using MEDLINE, EMBASE and Cochrane Central Register of Controlled Trials (CENTRAL), encompassing studies from inception to December 2024. The primary outcome was in-hospital mortality in KTR undergoing PCI compared with non-KTR cohorts. A random-effects model was used to analyse pooled data. A total of six studies with 13,287,090 patients were included. Four studies compared PCI outcomes in KTR with various degrees of renal dysfunction, revealing significantly lower in-hospital mortality in KTR compared with patients with CKD (odds ratio [OR] 0.44, 95% confidence interval [CI] 0.35 to 0.55, p<0.001). No significant difference was seen in in-hospital mortality between KTR and patients without CKD (OR 1.12, 95%CI 0.75 to 1.68, I2=95.60%, p=0.57). Two studies compared KTR and patients on haemodialysis, both observed a lower incidence of MACE in the KTR group compared with the haemodialysis cohort (OR 0.43, 95%CI 0.20 to 0.92, I2=0%, p=0.03). In conclusion, PCI in KTR is associated with lower in-hospital mortality as compared with patients with CKD or those on dialysis. There was no mortality difference observed when comparing KTR with patients without CKD.
Introduction
Chronic kidney disease (CKD) is a well-established risk factor for cardiovascular disease, associated with significantly increased morbidity and mortality.1 People with CKD often have multiple cardiovascular risk factors, including hypertension, diabetes mellitus and hyperlipidaemia. In addition to these traditional risk factors, CKD induces a pro-inflammatory state, which contributes to pathological myocardial remodelling, fibrosis, atherosclerosis and endothelial dysfunction. Further, associated disturbances in mineral metabolism including hyperphosphataemia and hyperparathyroidism lead to accelerated vascular calcification.2 Consequently, coronary artery disease (CAD) is highly prevalent in this population.
Kidney transplantation has been shown to mitigate the progression of cardiovascular risk associated with CKD, primarily through improvements in kidney function and reduction of uraemic toxins. However, kidney transplant recipients (KTR) remain at elevated cardiovascular risk due to CKD-related factors and long-term immunosuppressive therapy, which can exacerbate hyperlipidaemia, diabetes and hypertension,3 increasing the risk of CAD progression and the need for percutaneous coronary intervention (PCI). Despite the growing population of KTR and high burden of cardiovascular morbidity, most large randomised-controlled trials evaluating PCI have historically excluded KTR. As a result, data on the efficacy and safety of PCI in this group remain limited, leaving clinicians to extrapolate management strategies from the general CKD or dialysis populations. Given the unique immunological considerations, potential drug interactions, and altered risk profiles of KTR, there is a pressing need for robust evidence to guide revascularisation strategies in this cohort.
Given the paucity of evidence about the efficacy and safety of PCI in KTR, this systematic review and meta-analysis aims to evaluate clinical outcomes associated with PCI in KTR, comparing them with individuals with CKD and those on dialysis undergoing PCI.
Method
A comprehensive search across multiple electronic databases from inception to December 2024 was conducted. Studies were included if they reported cardiovascular outcomes in KTR who had undergone PCI and provided comparative data with non-KTR cohorts. Exclusion criteria encompassed case reports, conference abstracts and studies reporting outcomes exclusively on coronary bypass surgery, as well as studies lacking comparative outcomes for KTR post-PCI. It was not possible to involve patients or the public in the design, analysis or reporting of this research project.
Title and abstract screening were conducted independently by two reviewers (IE and RB), followed by a full-text review of articles meeting initial eligibility criteria. Any discrepancies were resolved through discussion with a third reviewer (ANK). Data from included studies were extracted to capture study characteristics, patient demographics, details of PCI, and clinical outcomes. The primary end point for this analysis was in-hospital mortality.
Odds ratios (OR) and 95% confidence intervals (CI) for in-hospital mortality and major adverse cardiovascular events (MACE) were either derived directly from studies, or manually calculated from raw data. Meta-analysis was conducted using a random-effects model to account for potential heterogeneity across studies, with heterogeneity assessed with the I2 statistic. I2 values of 25%, 50% and 75% were considered as indicating low, moderate, and high heterogeneity, respectively. Statistical significance was set at p<0.05.
Results
Following removal of duplicates, title and abstract screening and full-text screening, six studies met all criteria and were included for analysis.4–9 All six studies were retrospective and were conducted across diverse geographic locations, with substantial variation in sample size and study design (table 1). The largest study had 5,811,026 patients. Four studies examined outcomes following PCI in KTR compared with patients with CKD at various stages; two of these also analysed patients with normal kidney function. The final two studies compared KTR and patients undergoing haemodialysis. Only one study matched for baseline characteristics.6 Notably, no randomised-controlled trials were identified.
Table 1. Qualitative analysis and characteristics of included studies
| Author (year) | Study design | Country (time period) | Total population | KTR population; mean age in years; % male | Primary outcome |
| Gupta et al. (2017)4 | Retrospective cohort study | United States (2003–2013) | 352,054 | 2,980; 57.5 ± 11.1; 72.7% |
In-hospital mortality: 8.5% vs. non-CKD, 8.4% vs. 23.5% stage 5D CKD |
| Agrawal et al. (2016)5 | Retrospective cohort study | United States (2003–2011) | 5,811,026 | 9,243; 58.2 ± 11.1; 66% | In-hospital mortality: NSTEMI 2.5% vs. 8.8% CKD vs. 4.2% non-CKD/KTR; STEMI 8.8% vs. 23.5% CKD vs. 8.8% non-CKD/KTR |
| Nakao et al. (2020)6 | Retrospective cohort study | Japan (2002–2017) | 100 | 50; 58.5 ± 9.1; 72% | Incidence of MACE-free rates: 1-year 81.6% vs. 65.0% HD; 3-year 70.5% vs. 46.2% HD 5-year 64.1% vs. 40.5% HD |
| Rashid et al. (2021)7 | Retrospective cohort study | United States (2004–2014) United Kingdom (2007–2014) |
US: 6,601,526 UK: 515,408 |
US: 12,529; 57.93 ± 0.21; 67.37% UK: 1,521; 61 (interquartile range 53–70); 73.8% |
US study In-hospital mortality: 2.16% KTR vs. 1.61% no KTR UK study All-cause mortality: 30 days 3.0% vs. 2.0% no KTR and 1 year 7.6% vs. 4.8% no KTR |
| Borentain et al. (2005)8 | Retrospective cohort study | France (1995–2001) | 224 | 37; 52 ± 10; 35% | In-hospital: Major cardiac events: 5% vs. 5% control vs. 9% dialysis Death: 0 (n) vs. 0 control vs. 1 dialysis Vascular complication: 2 (n) vs. 1 control vs. 2 dialysis Blood transfusion: 2 (n) vs. 1 control vs. 1 dialysis False aneurysm: 0 (n) vs. 0 control vs. 1 dialysis |
| Zheng et al. (2023)9 | Retrospective cohort study | Australia (2014–2021) | 16,752 | 226; 61 ± 10; 72% | 30-day major adverse cardiac and cerebrovascular events: 4.4% vs. 6.8% CKD vs. 11.6% dialysis |
| Key: CKD = chronic kidney disease; HD = haemodialysis; KTR = kidney transplant recipient; MACE = major adverse cardiovascular events; NSTEMI = non-ST-elevation myocardial infarction; STEMI = ST-elevation myocardial infarction | |||||
KTR were generally younger compared with non-KTR cohorts, although rates of comorbidities, including hypertension, diabetes mellitus, hypercholesterolaemia and previous coronary artery events, were higher. Among the four studies assessing PCI between KTR and patients with CKD, KTR demonstrated a significantly lower in-hospital mortality rate compared with patients with CKD (OR 0.44, 95%CI 0.35 to 0.55, p<0.001) with high heterogeneity (I2=80.93%) (figure 1). By contrast, no significant difference was seen in in-hospital mortality between KTR and patients without CKD (OR 1.12, 95%CI 0.75 to 1.68, I2=95.60%, p=0.57). Of the two studies comparing KTR and patients on haemodialysis, both observed a lower incidence of MACE in the KTR group compared with the haemodialysis cohort (OR 0.43, 95%CI 0.20 to 0.92, I2=0%, p=0.03).
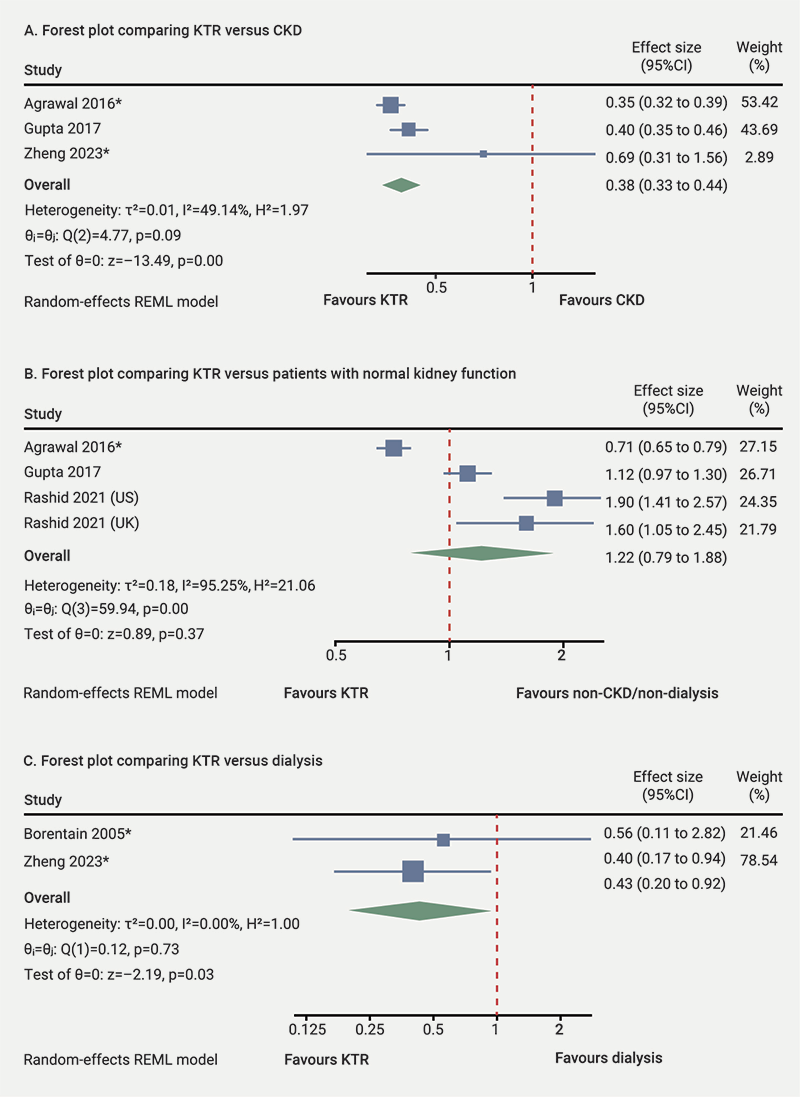
| *Asterisks denote manually calculated odds ratios (ORs) Key: CI = confidence interval; CKD = chronic kidney disease; KTR = kidney transplant recipient; REML = restricted maximum likelihood |
Discussion
This systematic review of six heterogenous retrospective studies underscores the relative paucity of data examining PCI in KTR. Despite the limited evidence-base, our findings suggest that KTR may have a lower in-hospital mortality risk following PCI compared with both CKD and haemodialysis cohorts. These observations are particularly notable given that KTR, although younger, had higher rates of comorbidities, including hypertension, diabetes mellitus, hypercholesterolaemia, and previous coronary artery events.
Several mechanisms may account for the apparent survival advantage of KTR compared with non-transplant CKD or haemodialysis patients. First, once transplanted, patients are no longer subject to the large intravascular volume shifts inherent to dialysis, which can reduce haemodynamic stress and minimise acute cardiac strain. Additionally, improved kidney function may reduce electrolyte imbalances and slow progression of arterial calcification, thereby mitigating some drivers of coronary disease. A decline in chronic inflammation and atherosclerosis after kidney transplantation – linked to better clearance of uraemic toxins – may also contribute to more stable coronary lesions, potentially rendering PCI less complex. Furthermore, KTRs are judiciously selected and typically suffer from fewer comorbidities, which may potentially contribute to improved PCI outcomes. Nonetheless, it is important to recognise that kidney transplantation introduces its own risks. Long-term immunosuppressive therapy can exacerbate metabolic disturbances and may perpetuate a degree of inflammation.2–6 These factors could, in theory, offset some of the survival benefits gained by improved kidney function. Additionally, patients remaining on dialysis, or those with advanced CKD, may have been deemed ineligible for transplantation due to higher baseline comorbidity burdens, further amplifying differences in outcomes.
Of particular interest, we found no significant difference in in-hospital mortality between KTR and patients without CKD. This finding, though based on limited data, suggests that some of the excess risk conferred by advanced CKD may be reversible following kidney transplantation. Such a conclusion is cautiously optimistic, indicating that coronary interventions in KTR can achieve outcomes similar to the general population with normal kidney function – albeit with continued vigilance regarding immunosuppressive-related risks.
The main limitation of our study was the lack of randomised data. All studies were observational, with unadjusted confounding factors and selection bias. Although five studies attempted to adjust for confounders,4,5,7–9 the variables used and their definitions varied considerably, contributing to the heterogeneity observed in the meta-analysis.
Conclusion
KTR undergoing PCI appear to have a lower risk of in-hospital mortality than patients with CKD or those on dialysis, likely reflecting the benefits of improved kidney function and reduced uraemic burden. Further prospective studies focusing on KTR are essential to confirm these results and refine clinical strategies for improving outcomes in this unique and high cardiovascular risk population.
Key messages
- Outcomes following percutaneous coronary intervention (PCI) for kidney transplant recipients are limited
- This systematic review and meta-analysis aims to evaluate clinical outcomes in this cohort, compared with individuals with chronic kidney disease and those on dialysis
- The aim of this research is to help guide management strategies in kidney transplant recipients
Conflicts of interest
None declared.
Funding
None.
References
1. Zoccali C, Mallamaci F, Adamczak M et al. Cardiovascular complications in chronic kidney disease: a review from the European Renal and Cardiovascular Medicine Working Group of the European Renal Association. Cardiovasc Res 2023;119:2017–32. https://doi.org/10.1093/cvr/cvad083
2. Nelson AJ, Raggi P, Wolf M, Gold AM, Chertow GM, Roe MT. Targeting vascular calcification in chronic kidney disease. JACC Basic Transl Sci 2020;5:398–412. https://doi.org/10.1016/j.jacbts.2020.02.002
3. Kramer BK, Zulke C, Kammerl MC et al. Cardiovascular risk factors and estimated risk for CAD in a randomized trial comparing calcineurin inhibitors in renal transplantation. Am J Transplant 2003;3:982–7. https://doi.org/10.1034/j.1600-6143.2003.00156.x
4. Gupta T, Kolte D, Khera S et al. Management and outcomes of ST-segment elevation myocardial infarction in US renal transplant recipients. JAMA Cardiol 2017;2:250–8. https://doi.org/10.1001/jamacardio.2016.5131
5. Agrawal S, Garg L, Garg A et al. Recent trends in management and inhospital outcomes of acute myocardial infarction in renal transplant recipients. Am J Cardiol 2017;119:542–52. https://doi.org/10.1016/j.amjcard.2016.10.041
6. Nakao M, Yamaguchi J, Satomi N et al. Outcomes of renal transplant recipients after percutaneous coronary intervention. Am J Cardiol 2020;125:1305–11. https://doi.org/10.1016/j.amjcard.2020.02.007
7. Rashid M, Nagaraja V, Shoaib A et al. Outcomes following percutaneous coronary intervention in renal transplant recipients: a binational collaborative analysis. Mayo Clin Proc 2021;96:363–76. https://doi.org/10.1016/j.mayocp.2020.04.045
8. Borentain M, Le Feuvre C, Helft G et al. Long-term outcome after coronary angioplasty in renal transplant and hemodialysis patients. J Interv Cardiol 2005;18:331–7. https://doi.org/10.1111/j.1540-8183.2005.00068.x
9. Zheng WC, Evans N, Dinh D et al. Clinical outcomes of renal transplant recipients undergoing percutaneous coronary intervention. Heart Lung Circ 2024;33:998–1008. https://doi.org/10.1016/j.hlc.2024.01.033
