Anxiety is common in people with coronary artery disease (CAD), particularly in association with invasive procedures and investigations. Effective provision of information for patients is crucial, but traditional methods may fail to adequately inform or engage some patients. We aimed to synthesise clinical trials evaluating the effectiveness of video animations provided to patients with CAD.
We performed a systematic review of Medline, CINAHL Plus, Cochrane Library and PsycINFO from January 2000 to January 2025. Conducted in accordance with PRISMA guidelines and presented with a narrative synthesis.
Five randomised-controlled trials met the inclusion criteria. Four included video animations, and one a ‘whiteboard animation’. Each evaluated the animations as an addition to standard care. Patient knowledge was improved in all four trials that assessed it, and anxiety was reduced in two out of four trials that assessed it. There was some evidence of beneficial effects of animations on satisfaction and health behaviours. The quality of evidence was not strong, with two trials having a high risk of bias.
In conclusion, video animations show potential for their effects on knowledge and anxiety in patients with CAD, but the evidence-base is small.
Introduction
Cardiovascular disease accounts for more than three million deaths in Europe annually, of which, coronary artery disease (CAD) is a leading cause.1 The burden of mortality and morbidity associated with CAD, and, in particular, acute coronary syndrome (ACS), is high. Effects on a patient’s lifestyle and self-image following ACS contribute to prevalence rates of 12–15% for depression and 10–38% for anxiety.2 Anxiety and depression are common in patients with cardiovascular disease,3 and are associated with disadvantaged clinical outcomes following ACS.4
The importance of psychological care for patients with life-threatening conditions is increasingly recognised. For patients with CAD, this may include preparation for invasive procedures, such as angiography, and for hospital discharge. Face-to-face provision of information is important for preparing patients and gaining informed consent, and has traditionally been supplemented by information leaflets and online resources. However, patients may not always understand what is being explained,5 particularly among non-native language speakers and those with lower levels of health literacy. Indeed, a ‘high information burden’ (that is, information that is lengthy, complex or poorly written) may deter engagement by patients, either because it is hard to understand or perceived as such.6
Providing information through videos, including video animations, may be more accessible and engaging for patients, and is associated with greater patient engagement and satisfaction,5,7 and image-based information (whether static or animated) can increase patients’ understanding of their health condition more than words alone. Graphics and animations may also enhance patients’ understanding and factual knowledge of specific healthcare interventions.8,9 However, little is known about the impact of these technologies on anxiety and knowledge in patients with CAD.
The aim of this systematic review is to synthesise trials that evaluate the effectiveness of video animations provided to patients with CAD.
Method
The review was registered on PROSPERO (International Prospective Register of Systematic Reviews),10 and is reported in accordance with PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) guidelines.11
Inclusion and exclusion criteria
We included randomised- or quasi-randomised-controlled trials of patients with CAD examining video animations, when compared with standard care and/or another form of information provision (such as a booklet), and reporting anxiety or knowledge as an outcome. We included studies published from 2000, without geographical or language limits (and we translated potentially relevant articles not published in English).
Video animations were defined as video cartoons, animated 2D or 3D diagrams, film of avatars or ‘whiteboard animations’. We included animations being provided together with another intervention when the effect of the animation could be isolated, or when the animation formed the main part of the intervention.
Studies were eligible if they included participants with CAD (ST-elevation or non-ST elevation myocardial infarction, or unstable angina), ischaemic heart disease, cardiovascular disease, or undergoing coronary angiography, percutaneous coronary intervention (PCI) or coronary artery bypass graft (CABG). We excluded trials of hypothetical patients (for example, people being asked to imagine having ACS).
Data sources and searches
The search strategy was developed in Medline (Ovid) with the support of an information scientist and then adapted for other databases. Medline, Medline in-process, CINAHL Plus, Cochrane Library and PsycINFO were searched on 6 January 2025 (supplementary material figure 2 for Medline search), supplemented by the Open Grey database and backwards- and forwards-citation searches on Google Scholar.
Screening
Initially, titles and abstracts were screened independently by two reviewers (PS and PK), using pre-determined criteria. Potentially relevant full-text articles were independently screened by two authors (PS and PK). Disagreements at either stage were resolved through consensus discussion.
Data extraction and analysis
We created a form to undertake data extraction, which included: study title and aims, study design and analysis, and findings. Any information not reported was recorded as ‘not stated’.
In addition to the primary outcomes, we extracted data on attitudinal and behavioural outcomes (e.g. satisfaction with care, and adherence to treatment recommendation), and health outcomes (whether reported by patients, such as pain or return to work, or assessed by clinicians, such as blood pressure or perfusion).
Data were extracted by one author (PS) and then checked by a second author (PK), and findings were reconciled by consensus.
In view of the anticipated heterogeneity of the populations and outcomes, a narrative synthesis was planned.
Quality assessment
Included studies were appraised (by PS and then checked by PK) using the Cochrane ROB-2 tool for trials.12
Effect measures
The primary variables (anxiety and knowledge) were included as categoric or non-categoric (ordinal or interval) measures, and were compared across groups in the trials according to their incidence rates or mean values, respectively.
Synthesis
Data from the included trials were synthesised narratively.
Results
Of 762 unique citations, 30 full-text manuscripts were reviewed, of which, five met the inclusion criteria (figure 1).
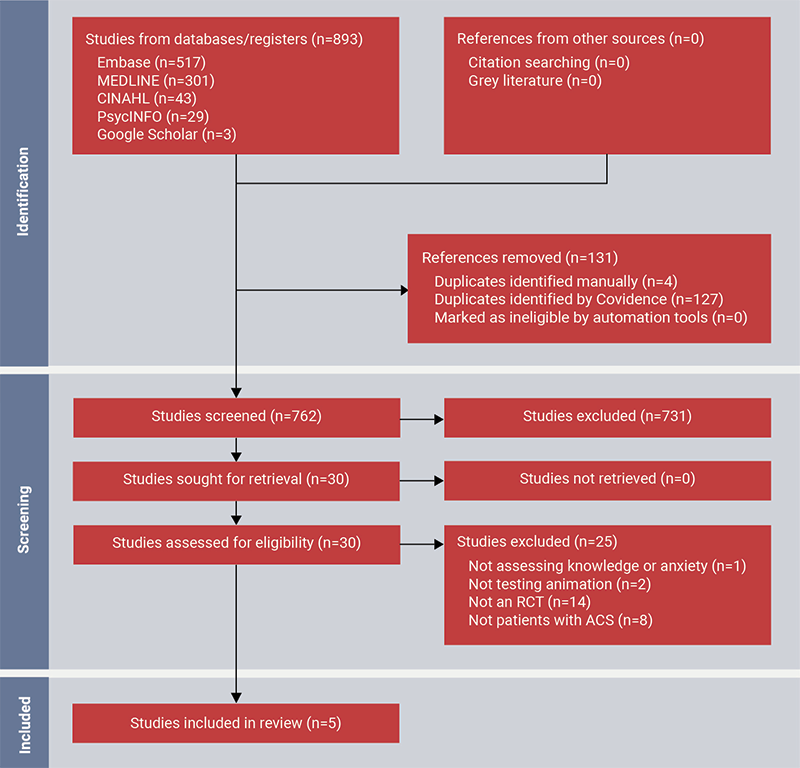
| Key: ACS = acute coronary syndrome; RCT = randomised-controlled trial |
Study characteristics
The five included studies were undertaken in Canada, France, Iran, New Zealand and Singapore, and were published between 2008 and 2024 (table 1).13–17 The studies tested the effectiveness of 3D animated video (three trials), 2D animated video (one trial) and ‘whiteboard animation’ (one trial).
Table 1. Details of included studies
| Study design | Setting | Participants, education level between the 2 groups | Mean age ± SD, years % male |
Sample size Intervention descriptor Control descriptor |
Intervention details | Results (intervention vs. control) | Group favoured | ||
| Knowledge | Anxiety | Behaviours/ satisfaction/ health outcomes | |||||||
| Yap et al., 2020, Singapore13 * | |||||||||
| RCT | 1 tertiary centre hospital | Patients undergoing coronary angiography and angioplasty Education NS |
59.1 ± 9.9; NS 84%; NS |
N=332 I=252 Animated educational video + traditional written educational pamphlet and standard physician counselling C=80 Traditional written educational pamphlet and standard physician counselling |
3-minute animated video (white board animation), describing indications, events, risks and benefits of procedure + usual care Watched once on smart phones, tablets and computers |
Mean score out of 12 ± SD: Pre-I: 7.6 ± 3.1 Post-I: 10.2 ± 1.7 C: 8.5 ± 2.9 Pre-I vs. Post-I p≤0.001 Post-I vs. C p≤0.001 |
STAI test ± SD (40–160): Pre-I: 93.5 ± 14.2 Post-I: 74.9 ± 19.1 C: 91.8 ± 12.7 Pre-I vs. Post-I p≤0.001 Post-I vs. C p≤0.001 |
Heart rate ± SD: Post-I: 70.2 ± 11.7 C: 70.5 ± 12.7 p=NS Systolic BP: Post-I: 132.6 ± 18.5 C: 132.7 ± 17.4 p=NS Diastolic BP: I: 79.0 ± 10.3 C: 79.3 ± 9.2 p=NS |
Knowledge Favours animation Anxiety Favours animation Health outcomes No differences between groups |
| Lattuca et al., 2018, France14 ** | |||||||||
| RCT | 39 coronary intervention centres | Patients undergoing coronary angiography and angioplasty Education NS |
67.3 ± 11.6; NS 72% (I 75%; C 68%); p=0.02 |
N=821 I=406 Animated educational video + standard spoken and written information C=415 Standard spoken and written information |
5-minute 3D animated video describing indications, events, risks and benefits + usual care Watched on a tablet in the presence of research assistant, questions on the video were deferred until completion of questionnaire |
16-point scale, mean ± SD: I: 11.8 ± 2.8 C: 9.5 ± 3.1 I vs. C p≤0.001 Knowledge was higher in subgroup analysis regarding procedure, long-term management, complications, education levels and age (p<0.001 for all) |
10-point scale, mean ± SD: I: 3.2 ± 2.7 C: 3.5 ± 3.0 NS |
Knowledge Favours animation Anxiety No difference between groups |
|
| Bowers et al., 2015, Canada15 | |||||||||
| RCT | 1 hospital | Patients undergoing angioplasty (n=28), EVAR (n=25), PICC (n=20) and Hickmann (n=20) Education NR |
60.9 (range 19–89)# 62.5% |
N=93 I=49 Animated video + standard care C=44 Standard care |
2-minute computer-generated video for each procedure Described the anatomy, instruments and procedure. No audio Video was viewed once on iPads |
5 true/false questions 2 x 4 ANOVA was conducted I vs. C: F=9.14, p=0.003 No differences according to conducted surgical procedure |
Not measured | Satisfaction with consent process: 6 questions using a 1–5 scale (possible range 6–30) I vs. C: F=44.06, p≤0.001 No differences according to conducted surgical procedure |
Knowledge Animation improved knowledge Satisfaction Favours animation |
| Oudi et al., 2024, Iran16 | |||||||||
| RCT | 1 heart centre | Patients undergoing angiography Education NR |
C: 63.0 ± 11.2 VR: 56.9 ± 14.3 EV: 59.6 ± 13.7 NS C: 50% VR: 50% EV: 70% NS |
N=90 EV=30 3D animated video VR=30 Virtual-reality distraction C=30 Routine care |
Education video included 5-minute 3D animation about the procedure (no other details provided) Virtual reality was a 5-minute distraction with a natural scene, such as beaches, mountains, waterfall with soothing sounds |
Not measured | STAI test ± SD (40–160) Overt anxiety: EV: 38.1 ± 8.6 C: 40.4 ± 9.6 NS Covert anxiety: EV: 34.8 ± 8.5 C: 43.0 ± 9.9 NS |
Anxiety: No difference between groups |
|
| Jones et al., 2016, New Zealand17 | |||||||||
| RCT | 1 hospital | Patients admitted for ACS Education NR |
60.9 ± 10.2; NS 70%; NS |
N=70 I=35 (31 analysed) Animated video plus standard care C=35 (30 analysed) Standard care |
15-minute animated video in two parts: (i) relevant anatomy, pathophysiology and effects of ACS; (ii) health protective behaviours and how medications work Information was given on iPads. Watched once |
Identifying medication adherence as a heart-healthy behaviour (7 weeks post-intervention): I: 55% (18/33) C: 29% (9/31) p=0.039 NS difference between groups for naming other healthy behaviours |
Cardiac Anxiety Questionnaire Animation group had lower anxiety scores C: adjusted mean 8.9 (95%CI 7.3 to 10.4) I: adjusted mean 6.6 (95%CI 5.0 to 8.1) C vs. I: F=4.50, p=0.038 |
Number of days to return to activity: I=17.4 days C=20.7 days p=0.043 Number of days to return to paid work: I=21.4 days C=22.9 days NS |
Knowledge Favours animation in 1 aspect (out of 4) of knowledge of healthy behaviours No difference between groups on the other 3 behaviours Anxiety Favours animation Behaviour Favours animation on return to activity No difference between groups on return to paid work |
| * Link to animated educational video: https://youtu.be/R8AdaIbNq7Y ** Animated vídeo available from: https://www.sciencedirect.com/science/article/pii/S0002870318300784#s0085 (suppl 1) # Standard deviation not reported. Key: ACS = acute coronary syndrome; ANOVA = analysis of variance; BP = blood pressure; CI = confidence interval; EV = educational video; EVAR = endovascular aneurysm repair; C = control; I = intervention; NR = not reported; NS = not significant; PICC = peripherally inserted central catheter; Pre-I = pre-intervention; Post-I = post-intervention; RCT = randomised-controlled trial; SD = standard deviation; STAI = State-Trait Anxiety Inventory; VR = virtual reality |
|||||||||
In total, there were 1,466 participants in the five trials (trial sample range 70 to 821), with a mean age of 61.6 years and 71.9% being male.
Participants were scheduled to undergo coronary angiography and angioplasty (two trials) or angiography (one trial). In one trial, patients were having one of several invasive procedures (angioplasty, endovascular aneurysm repair, Hickmann line insertion or peripherally inserted central catheter insertion). In another trial, patients had been admitted to hospital with ACS.
Risk of bias in studies
The included studies had mixed scores on the quality appraisal checklist (table 2): overall two of the trials were rated as having high risk of bias, and three were rated as ‘some concerns’. Trials scored well on ‘randomisation process’ and ‘deviations from intended interventions’ but were weak on ‘measurement of the outcome’.
Table 2. Quality rating of included trials (on the Cochrane ROB-2 tool)12
| Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported result | Overall risk of bias | |
| Bowers et al., 201715 | Low risk | Low risk | Low risk | Some concerns | Low risk | Some concerns |
| Jones et al., 201617 | Low risk | Some concerns | High risk | Some concerns | Low risk | High risk |
| Lattuca et al., 201814 | Low risk | Low risk | Low risk | Some concerns | Low risk | Some concerns |
| Oudi et al., 202416 | Low risk | Low risk | Low risk | Some concerns | Low risk | Some concerns |
| Yap et al., 201913 | Some concerns | Low risk | Low risk | High risk | Low risk | High risk |
Results of individual studies
Four of the five trials included anxiety outcomes, while four trials included knowledge outcomes. Three of the trials included behaviour, satisfaction or health outcomes.
Yap and colleagues13 tested a short ‘whiteboard animation’, which was provided in addition to standard spoken information from a physician and a printed booklet, when preparing patients for coronary angiography and angioplasty. Patients in the control group received only the spoken and written information. The intervention group had increased procedural knowledge and lower levels of anxiety than the control group. There was no difference between groups in recorded heart rate or blood pressure. In a subgroup analysis, the animation had similar levels of effectiveness in patients having their first or a subsequent angiogram.
Lattuca and colleagues14 evaluated a five-minute 3D animated video being provided in addition to standard spoken information to patients undergoing coronary angioplasty and angiography. Animation provision had no effect on anxiety levels but resulted in increased knowledge, both overall and on each of four subcomponents (the disease and its treatments; the procedure; potential complications; and what would happen in hospital). In a subgroup analysis, the animation improved knowledge in all four patient age groups and in all three education attainment groups.
Oudi and colleagues16 compared video animation with two alternatives: routine care and virtual reality (VR) distraction, given to patients undergoing angiography. Anxiety was the sole outcome measure, reported separately as overt and covert anxiety. The animation did not reduce overt or covert anxiety when compared with routine care or VR. VR reduced both forms of anxiety more than routine care.
Bowers and colleagues15 tested the effect of four animated videos, each lasting two minutes, about the interventional procedure the patient was being consented to. The videos, which did not include audio, conveyed the relevant anatomy, instruments used and procedure, and were provided in addition to standard verbal information to inform consent. The control group received verbal information only. The animations produced increased levels of knowledge and satisfaction with the consent process.
Jones and colleagues17 evaluated two animations about ACS that were given in addition to standard care (as received by patients in the control group). Videos covered healthy and unhealthy heart anatomy and physiology, and behaviours to maintain health, and were presented by a researcher who could also give clarification and answer questions. Still images were also shown to explain heart anatomy. Intervention group patients were given a link to view the videos at any time. Both groups in the study were asked to draw relevant heart anatomy, but only the intervention group was given feedback or had any misunderstandings corrected. The intervention reduced avoidance of cardiac anxiety and increased satisfaction with information. Intervention group patients were more likely to see medication adherence as a healthy behaviour, had increased belief in treatment benefits, increased perceived control, took less time to return to normal activities and took more daily exercise. There were no differences between groups in self-reported stress or heart-focused attention, or time to return to paid work.
Discussion
A summary of findings
The systematic review included five trials of animations being provided to patients with CAD. In the four trials with knowledge outcomes, animations produced increased knowledge compared with control group interventions in all four trials. In the four trials assessing anxiety, animations produced greater effects on anxiety or anxiety avoidance than the control group in two trials, but no difference in two trials. Animations increased satisfaction in both trials that assessed it, and behaviour outcomes were assessed in one trial, showing benefits from animations. Non-anxiety health outcomes were assessed in one trial, showing no difference between the intervention and control groups.
Strengths and limitations
The systematic review followed accepted good practice, to maximise retrieval of research and reduce bias. Good practice processes included: searching multiple databases, dual independent screening, checking of data extraction, quality appraisal of included studies, citation searching, and the inclusion of studies not reported in English (although in the end this process was not needed).
The overall evidence-base had the following positive features: anxiety was assessed by established measures, and animations were always provided in addition to standard information, protecting against non-specific information intervention effects. However, it also had some less positive aspects: there were only five trials, three of which had fewer than 100 participants each; the trials came from five countries, and so the evidence-base currently has little global reach; there were four single-centre trials, although the fifth trial involved 39 centres; and outcome measurement was short-term, with the longest follow-up being seven weeks post-intervention.
What does this study add?
This study adds to research evidence showing it is possible to provide patients with video or other digital forms of information,18 and that video animations tend to have positive effects on patients’ procedural or condition knowledge when provided in addition to standard information.18 As such, the review findings on CAD are consistent with the effects of animations given in a range of healthcare settings. This review also showed some positive effects of animations on patient attitudes and cognitions, which is consistent with the effects of animations more broadly.18 This is the first review to look at animations and anxiety outcomes, finding some evidence for positive effects.
Implications for practice
The evidence from the review is that patients with CAD are prone to anxiety and, in some cases, have knowledge deficits that should be met by practitioners and service providers; the evidence is that animations could contribute to that process. A concern sometimes voiced is that animations may be inappropriate for adult patients in healthcare settings because they are perceived by some as lacking in seriousness and can only achieve surface-level understanding of content.19,20 There was no evidence of those perceptions among the patients recruited to the five trials included here, and it is possible that the rapid growth in online health information over the past 15 years21 has removed any prior scepticism about information being delivered in something other than written or live spoken forms. Given the near universal access to digital technologies across the population in high- and middle-income countries,22,23 and the relatively low cost of commissioning and delivering a short animation, there are clear opportunities for services to provide effective animated information to patients with CAD.
Implications for research
There is a continued need for trials of animations, particularly larger, multi-centre trials, ideally including both short- and longer-term outcome measures. Furthermore, the evidence-base would be strengthened by less variation in animations, comparators and outcomes across trials, as this could open the possibility of statistical meta-analysis. This could be achieved by animations that have been evaluated positively, being evaluated again in subsequent trials, and trials using similar entry criteria and outcome measures, to facilitate meta-analysis.
Conclusion
Video animations show potential for their effects on knowledge and anxiety in patients with CAD, and there is no evidence of adverse effects on any of the outcome variables in the included trials, but the overall evidence-base is small.
Key messages
- This is the first systematic review of trials testing the effectiveness of video animations in coronary artery disease
- The review reports the five randomised-controlled trials to have compared an animation with another information intervention for patients
- The review shows that animations were more effective than the comparator at improving patient knowledge
- The review shows that animations were more effective than the comparator at reducing patient anxiety in two of the four trials that assessed it
Conflicts of interest
PS undertook work on the systematic review within an MB BS medical degree. PK, CW: none declared.
Funding
None.
Study approval
Research ethics approval was not required.
Acknowledgement
We thank Dr Helen Fulbright (CRD, University of York) for her guidance in developing the database searches.
Editors’ note
Supplementary materials are available on request.
References
1. Timmis A, Aboyans V, Vardas P et al. European Society of Cardiology: the 2023 atlas of cardiovascular disease statistics. Eur Heart J 2024;45:4019–62. https://doi.org/10.1093/eurheartj/ehae466
2. Mejía PJC, Cassano PD, Morón PD, Reátegui MD, Navarrete KM, Córdova-Mendoza P. Prevalence of anxiety and depression in patients with acute coronary syndrome: systematic review and meta-analysis. Pan Afr Med J 2023;46:91. https://doi.org/10.11604/pamj.2023.46.91.41792
3. Zeng J, Qiu Y, Yang C et al. Cardiovascular diseases and depression: a meta-analysis and Mendelian randomization analysis. Mol Psychiatry 2025;30:4234–46. https://doi.org/10.1038/s41380-025-03003-2
4. Eastwood J-A, Doering L, Roper J, Hays RD. Uncertainty and health-related quality of life 1 year after coronary angiography. Am J Crit Care 2008;17:232–42. https://doi.org/10.4037/ajcc2008.17.3.232
5. Beranova E, Sykes C. A systematic review of computer-based softwares for educating patients with coronary heart disease. Patient Educ Couns 2007;66:21–8. https://doi.org/10.1016/j.pec.2006.09.006
6. Von Wagner C, Semmler C, Good A, Wardle J. Health literacy and self-efficacy for participating in colorectal cancer screening: the role of information processing. Patient Educ Couns 2009;75:352–7. https://doi.org/10.1016/j.pec.2009.03.015
7. Fox MP. A systematic review of the literature reporting on studies that examined the impact of interactive, computer-based patient education programs. Patient Educ Couns 2009;77:6–13. https://doi.org/10.1016/j.pec.2009.02.011
8. Schnellinger M, Finkelstein M, Thygeson MV, Vander Velden H, Karpas A, Madhok M. Animated video vs pamphlet: comparing the success of educating parents about proper antibiotic use. Pediatrics 2010;125:990–6. https://doi.org/10.1542/peds.2009-2916
9. Leiner M, Handal G, Williams D. Patient communication: a multidisciplinary approach using animated cartoons. Health Educ Res 2004;19:591–5. https://doi.org/10.1093/her/cyg079
10. Knapp P, Sridhar P. The effectiveness of video animations in helping patients with acute coronary syndrome. Prospero 2025. Available from: https://www.crd.york.ac.uk/PROSPERO/view/CRD42025644193
11. Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg 2010;8:336–41. https://doi.org/10.1016/j.ijsu.2010.02.007
12. Sterne JAC, Savović J, Page MJ et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 2019;366:l4898. https://doi.org/10.1136/bmj.l4898
13. Yap J, Teo TY, Foong P et al. A randomized controlled trial on the effectiveness of a portable patient education video prior to coronary angiography and angioplasty. Catheter Cardiovasc Interv 2020;96:1409–14. https://doi.org/10.1002/ccd.28655
14. Lattuca B, Barber-Chamoux N, Alos B et al. Impact of video on the understanding and satisfaction of patients receiving informed consent before elective inpatient coronary angiography: a randomized trial. Am Heart J 2018;200:67–74. https://doi.org/10.1016/j.ahj.2018.03.006
15. Bowers N, Eisenberg E, Montbriand J, Jaskolka J, Roche-Nagle G. Using a multimedia presentation to improve patient understanding and satisfaction with informed consent for minimally invasive vascular procedures. Surgeon 2017;15:7–11. https://doi.org/10.1016/j.surge.2015.09.001
16. Oudi D, Mohammad Sadeghi A, Mohtasham S, Rajabi R, Eslami Aliabadi H. The effect of virtual reality and educational video on anxiety of cardiac angiography candidates: a randomized clinical trial. Evid Based Care 2025;14:58–66.
17. Jones ASK, Ellis CJ, Nash M, Stanfield B, Broadbent E. Using animation to improve recovery from acute coronary syndrome: a randomized trial. Ann Behav Med 2016;50:108–18. https://doi.org/10.1007/s12160-015-9736-x
18. Byrne TM, Knapp P, Lidster A et al. How effective are video animations as information tools for patients and the general public? An updated systematic review. Front Digit Health 2025;7:1717044. https://doi.org/10.3389/fdgth.2025.1717044
19. Mayer RE, Moreno R. Animation as an aid to multimedia learning. Educ Psychol Rev 2002;14:87–99. https://doi.org/10.1023/A:1013184611077
20. Paik ES, Schraw G. Learning with animation and illusions of understanding. J Educ Psychol 2013;105:278. https://doi.org/10.1037/a0030281
21. Jia X, Pang Y, Liu LS. Online health information seeking 9:1740. https://doi.org/10.3390/healthcare9121740
22. International Telecommunication Union. ITU releases 2018 global and regional ICT estimates. Available at: https://www.itu.int/en/mediacentre/Pages/2018-PR40.aspx
23. World Bank Group. World development report 2016: digital dividends. World Bank Publications, 2016. Available from: https://www.worldbank.org/en/publication/wdr2016
