Lipid management is a key component of secondary prevention after acute coronary syndrome (ACS), but guideline adherence is variable. Adjunctive lipid-lowering therapies (LLTs) beyond statins are available, yet eligibility in the real-world setting is not well-described. We aimed to improve local post-ACS lipid management, and evaluate eligibility for LLTs.
Consecutive admissions of patients with ACS to a district general hospital from April to June 2022 were assessed for: inpatient lipid-profile assessment, inpatient LLT management, and outpatient repeat lipid profiles. A structured intervention, including updating blood testing panels, education, and reference resources, was implemented. We re-audited admissions in April–June 2024, where eligibility for adjunctive LLTs was assessed.
There were 97 (cycle 1) and 102 (cycle 2) patients identified. While performance was suboptimal in cycle 1, we observed improvements in cycle 2 (baseline full lipid profile testing from 10% to 75%; appropriate LLT management 65% to 78%; post-discharge repeat testing 37% to 63%). At one year post-ACS, 35% of patients remained subtherapeutic, but medication changes were rare.
In conclusion, through use of a structured intervention, we were able to improve post-ACS lipid management. Many patients fail to achieve therapeutic lipid lowering. Strategies to address this are urgently required.
Introduction
Ischaemic heart disease is the leading cause of death globally, responsible for 13% of all deaths in 2021.1 Acute coronary syndrome (ACS) represents a key opportunity for secondary prevention to reduce the risk of recurrent cardiovascular (CV) events.2 Lipid-lowering therapy (LLT) is central to this, with elevated levels of low-density lipoprotein cholesterol (LDL-C) being a key initiating factor in atherosclerosis:3 every 1 mmol/L reduction is associated with an approximate 22% decrease in the risk of major CV events.4 For patients with ACS, the National Institute for Health and Care Excellence (NICE) recommends:5,6
- Early initiation of high-intensity statin (HIS) therapy (atorvastatin 80 mg or equivalent).
- Measurement of a baseline lipid profile, including non-high-density lipoprotein cholesterol (non-HDL-C).
- Repeat lipid assessment three months post-discharge to ensure an adequate response to treatment, defined as either a >40% reduction in non‑HDL‑C or an absolute level ≤2.5 mmol/L.
Historical real-world data show that adherence to NICE guidance is variable, particularly in relation to lipid evaluation on admission, and follow-up after discharge.7,8 Locally, we identified that the default blood test panel for patients in the emergency department (ED) with suspected ACS measured only total cholesterol, rather than a full lipid profile including HDL-C, non-HDL-C, LDL-C and triglycerides. Although reasons for poor community-based reassessment may vary by region, we anecdotally observed inconsistent discharge communications with primary care, and hypothesised that this could contribute to inadequate lipid reassessment. NICE provides recommendations for discharge letters, specifying that the diagnosis, results of investigations, incomplete drug titrations, future management plans, and advice on secondary prevention, should be included in every summary.9
Traditionally, patients who failed to achieve therapeutic lipid modification could be offered ezetimibe as add-on therapy.5,6 In recent years, further LLTs have been developed, including proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors, such as the monoclonal antibodies alirocumab and evolocumab,10,11 and inclisiran, a small-interfering (si) RNA.12 Icosapent ethyl (IPE), a purified ethyl ester of eicosapentaenoic acid, lowers triglyceride levels, and may also offer anti-inflammatory and plaque-stabilising benefits.13 With the exception of inclisiran, these agents have demonstrated reductions in adverse CV events in clinical trials.10,11,14 Consequently, they are recommended for patients with persistently elevated LDL-C or hypertriglyceridaemia despite maximally tolerated statin therapy (table 1).15,16 However, eligibility for these treatments among patients with ACS is not well-characterised in the real-world setting in the UK.
Table 1. Current indications for adjunctive lipid-lowering therapies in patients with established cardiovascular disease. Based on National Institute for Health and Care Excellence (NICE) technology appraisals
| Agent | Indications | |
| Alirocumab, evolocumab | Mixed hyperlipidaemia: LDL-C >4.0 mmol/L Familial hypercholesterolaemia: LDL-C >3.5 mmol/L In the context of maximally tolerated lipid-lowering therapy |
|
| Inclisiran | LDL-C >2.6 mmol/L despite maximally tolerated lipid-lowering therapy | |
| Icosapent ethyl | Established on statin therapy with controlled LDL-C (1.04–2.60 mmol/L) but persistent hypertriglyceridaemia (≥1.7 mmol/L) | |
| Bempedoic acid (combination with ezetimibe) |
Statin contraindication or intolerance, with insufficient LDL-C control on ezetimibe monotherapy | |
| Key: LDL-C = low-density lipoprotein-cholesterol | ||
Here, we aimed to: improve lipid management following ACS, in line with NICE guidance; and assess downstream eligibility for adjunctive LLTs after ACS in a real-world, high-risk cohort.
Method
We conducted a retrospective two-cycle quality improvement project (QIP) at a district general hospital (Great Western Hospital [GWH], Swindon). The project was registered and approved locally (DOM-053/1, DOM-054/1).
Study design
We evaluated lipid management in patients admitted with ACS to GWH, identified by national audit submissions. Consecutive patients admitted over a three-month period were included. Patients directly transferred to another centre for percutaneous coronary intervention (PCI), with non-type 1 ACS events, out-of-area residency (defined as a non-SN postcode, to allow community follow-up through linked general practice records), who self-discharged, died during admission, or were placed on an end-of-life care pathway, were excluded.
The QIP was structured using a ‘plan-do-study-act’ model. Cycle 1 comprised a baseline observational audit of consecutive admissions between April and June 2022. Following analysis, a series of interventions were implemented, followed by re-audit of outcomes between April and June 2024:
- Local ‘chest pain’ bloods panel: we modified the local default panel, from only testing total cholesterol, to inclusion of a full lipid profile (including non-HDL-C and LDL-C).
- Departmental LLT management guide: we developed a guide for internal departmental use, based on NICE guidelines, to provide clinicians with an easy-to-access reference document.
- Standardised ACS discharge template: we created a template discharge letter, to ensure provision of consistent secondary prevention advice, including lipid targets and an escalation plan for LLT.
- Education sessions for resident doctors.
Outcomes, data collection and analysis
Two authors (ML, P-TT) retrospectively reviewed electronic patient records. Baseline characteristics were collated, including age, gender, and the presence of CV risk factors. Baseline lipid assessment was reviewed, alongside admission LLT and inpatient changes to therapy. Discharge doses of LLT and completeness of secondary prevention information were obtained from discharge summaries. Linked community records and biochemistry systems were used to assess for repeat lipid-profile testing, and community changes to LLT.
Quality metrics were evaluated in line with NICE guidance, as outlined above. Five domains were assessed:
- Admission lipid assessment: we reviewed admission assessment of lipid profiles, including whether this was performed, and whether non-HDL-C was measured.
- Inpatient LLT management: inpatient optimisation of LLT was assessed according to admission therapy, categorising patients into three groups: LLT-naïve, those on HIS therapy (defined by NICE guidance as any LLT with an expected ≥40% LDL-C lowering capacity), and those on other forms of LLT, such as ezetimibe. For patients not on maximal-dose HIS, appropriate management was defined as initiation or escalation to atorvastatin 80 mg (or equivalent), unless contraindicated. For patients already on maximal-dose HIS, appropriate management was judged based on achievement of lipid targets and the clinical context, including comorbidities and history of recurrent CV events.
- Discharge summary information: we reviewed discharge summaries to ensure consistent documentation of a minimum set of information regarding patient admission (diagnosis and management undertaken), lipid-specific secondary prevention (targets, escalation plans), other secondary prevention targets (antiplatelet plan including agents and duration, blood pressure targets, smoking cessation advice for smokers), and other important patient information (driving restrictions).
- Outpatient lipid reassessment: repeat profiling was deemed acceptable if performed within four months of discharge; whether the panel included a non-HDL-C measurement was also assessed.
- Eligibility for adjunctive agents: this was not assessed in cycle 1 as this lay outside of the scope of the initial audit, where our primary aim was to capture local practice and identify areas for improvement, but was performed in cycle 2 in accordance with NICE recommendations (TA733 and TA805; table 1).
Data are expressed as mean ± standard deviation (SD) or number (percentage). Statistical analyses comparing the performance in quality metrics across the two cycles were conducted using two-tailed Chi-square tests; a p value <0.05 was considered statistically significant.
Results
There were 199 patients identified: 97 in cycle 1 and 102 in cycle 2. Baseline demographics were comparable between cohorts (table 2).
Table 2. Baseline characteristics
| Characteristic | Cycle 1 (n=97) |
Cycle 2 (n=102) |
||
| Mean age ± SD, years | 67.7 ± 13.5 | 69.6 ± 12.6 | ||
| Female, n (%) | 29 (30) | 32 (31) | ||
| Admission LLT | HIS, n (%) | 41 (42) | 51 (50) | |
| Non-HIS, n (%) | 8 (8) | 10 (10) | ||
| No LLT, n (%) | 48 (49) | 41 (40) | ||
| Cardiovascular risk factors | Known CVD, n (%) | 41 (42) | 45 (44) | |
| Hypertension, n (%) | 56 (58) | 67 (66) | ||
| Smoking history, n (%) | 52 (54) | 45 (44) | ||
| Diabetes mellitus, n (%) | 28 (29) | 31 (30) | ||
| Admission lipid profile, mean ± SD, stratified by baseline therapy |
HIS | Total cholesterol | 4.0 ± 1.3 | 4.2 ± 1.4 |
| Non-HDL-C | 3.6 ± 2.5* | 2.9 ± 1.3 | ||
| Non-HIS | Total cholesterol | 5.0 ± 1.2 | 4.7 ± 1.5 | |
| Non-HDL-C | N/A† | 3.3 ± 1.4 | ||
| No LLT | Total cholesterol | 5.8 ± 1.3 | 5.9 ± 1.2 | |
| Non-HDL-C | 4.0 ± 0.9‡ | 4.6 ± 1.0 | ||
| High-intensity statin as defined by National Institute for Health and Care Excellence (NICE), i.e. agent and dose with ≥40% LDL-C lowering capacity. * Based on three results only. † No results. ‡ Based on seven results only. Key: CVD = cardiovascular disease; HDL-C = high-density lipoprotein-cholesterol; HIS = high-intensity statin; LLT = lipid-lowering therapy; SD = standard deviation |
||||
Cycle 1: April–June 2022
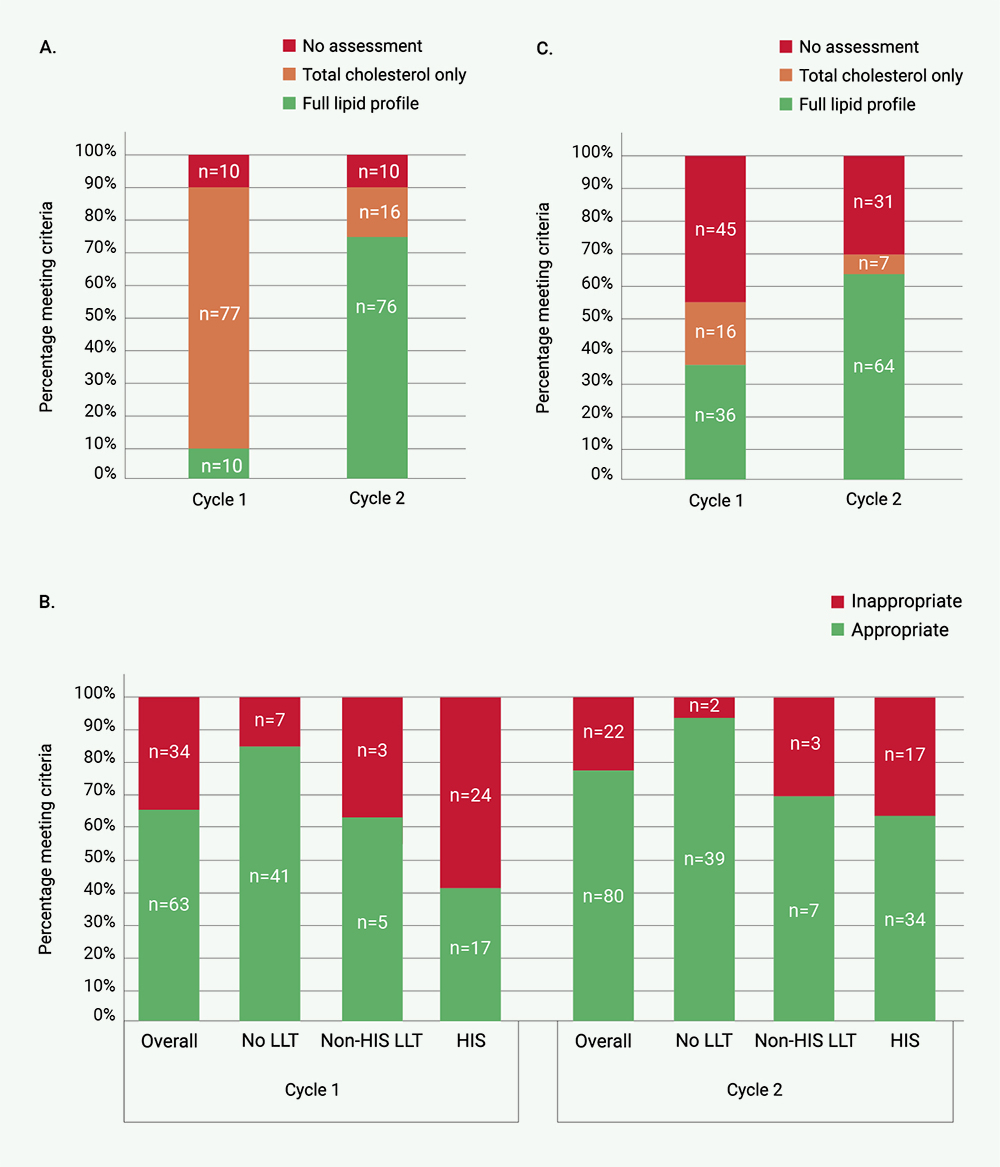
Initial audit revealed that only 10% of patients had a full lipid profile on admission, with the large majority having solely a total cholesterol assessment (figure 1A).
Inpatient LLT management was deemed appropriate for 65% (63/97) of patients (figure 1B). Appropriate LLT management was best performed in those not on any LLT on admission (41/48, 85%), followed by patients on non-HIS LLT (5/8, 63%), and finally those on HIS on admission (17/41, 41%).
Discharge letters contained suboptimal information for ongoing management in primary care: no letters contained any documented lipid targets, and only 3% (3/97) outlined an escalation plan for LLT. After discharge, 54% (52/97) of patients had repeat lipid testing, although only 69% of these (36/52) had reassessment with a profile including non-HDL-C measurement (figure 1C).
| Key: HIS = high-intensity statin; LLT = lipid-lowering therapy |
Cycle 2: April–June 2024
After the interventions described above, we repeated our audit of performance in lipid assessment and LLT management. Following the update to our ‘chest pain’ blood care set, we observed a significant increase in the proportion of patients with a full lipid profile on admission, to 75% (76/102, p<0.001) (figure 1A). However, 10% of patients still did not undergo lipid testing on admission: review of individual cases demonstrated that these were patients with ACS not admitted via the ED, as the updated blood testing panel was primarily used by the ED.
With improved admission lipid testing and initiatives to enhance local awareness of LLT management, we also observed improved inpatient LLT optimisation, across all levels of baseline LLT therapy (figure 1B). As previously, patients not on LLT at admission were the group with the highest rate of appropriate management: this rose to 95% (39/41). Improvements were also observed for patients on non-HIS LLT (70%, 7/10), and HIS (67%, 34/51). This resulted in a modest, but statistically significant, improvement in overall appropriate management of LLT: 63/97 (65%) to 80/102 (78%), p=0.04.
Post-discharge repeat lipid testing improved to 70% (71/102), with 90% (64/71) including non-HDL-C assessment. Overall, this represented a significant improvement in repeat full lipid testing across the cohort compared with cycle 1 (64/102 vs. 36/97, p<0.001) (figure 1C).
Finally, as part of our intervention, we produced a standardised ACS discharge letter template. Although this was only used in 22% (22/102) of cases, it appeared to drive an increase in the proportion of discharge letters containing secondary prevention lipid information (26%). In addition, exploratory analysis suggested that its use was associated with a significantly higher likelihood of repeat testing that included non-HDL-C measurement: 19/22 (86%) versus 45/79 (57%) without the template, p=0.01.
Achievement of therapeutic lipid targets, and use and theoretical eligibility for adjunctive LLTs
Patients in cycle 2 were followed-up for up to one-year post-discharge: 89% (91/102) underwent repeat lipid assessment by this time; of these, 93% (85/91) included non-HDL-C measurement. On the first repeat non-HDL-C measurement, 35% (30/85) of patients remained subtherapeutic (non-HDL-C >2.5 mmol/L).
The last recorded lipid profile was assessed to determine therapeutic target achievement, trends in LLT management (including ezetimibe use), and theoretical eligibility for inclisiran and IPE. At one year, 41% (35/85) remained subtherapeutic. Ezetimibe was prescribed in 14 patients in total, but rarely commenced as an outpatient after ACS admission for subtherapeutic LLT: this was only performed in four cases, with six on ezetimibe on admission, and four commenced during inpatient admission with ACS. Indeed, medication optimisation was uncommon: 91% (32/35) of patients with subtherapeutic lipid profiles appeared to have no change in dispensed LLT prescriptions between discharge and last follow-up.
Two patients were theoretically eligible for inclisiran (figure 2A), and 10 for IPE (figure 2B), though this was only prescribed in one patient. Accounting for patients who did not undergo repeat testing, the estimated theoretical eligibility for inclisiran in this population was 5%, and 18% for IPE.
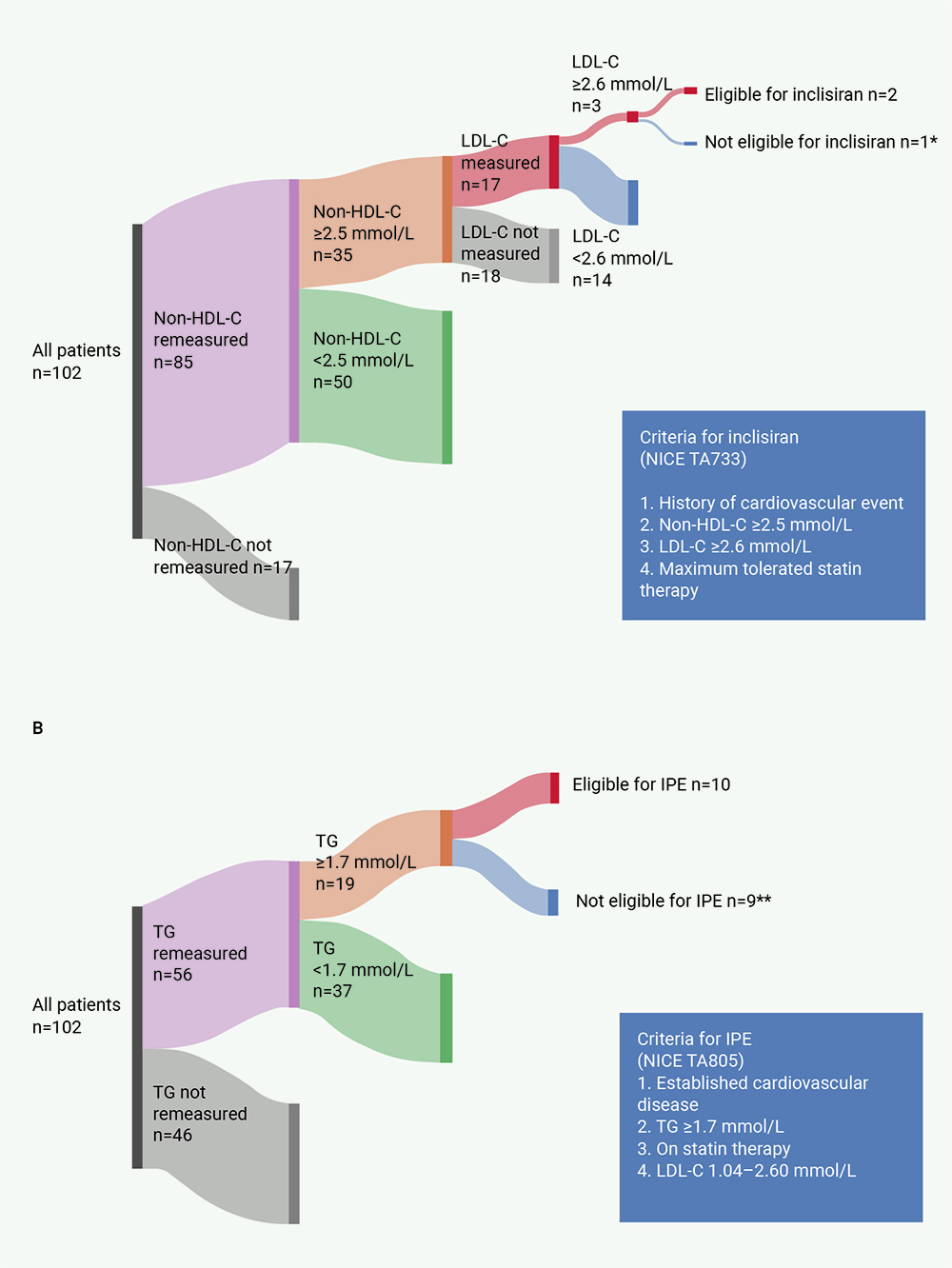
| *Patient on a moderate-intensity statin, with no discernible contraindication to escalation to a high-intensity statin. **5 due to LDL-C out of range; 4 no LDL-C on record. Eligibility assessment based on last available full lipid profile. Key: HDL-C = high-density lipoprotein-cholesterol; IPE = icosapent ethyl; LDL-C = low-density lipoprotein-cholesterol; NICE = National Institute for Health and Care Excellence; TG = triglycerides Made using SankeyMATIC (https://sankeymatic.com/build/). |
Discussion
Here, we report performance in lipid management in patients with ACS at a district general hospital. After structured intervention, consisting of changes to blood testing infrastructure, creation of resources for doctors, and education, we observed improvements in all audited areas, including admission lipid assessment, inpatient LLT management, discharge communication, and outpatient reassessment. Furthermore, we report the theoretical eligibility of this population for inclisiran and IPE.
Improving lipid-management pathways
We report the results of our multi-faceted approach towards improving local lipid management, including system interventions (updating bloods panel), and local educational sessions, supplemented by resources to drive sustainable improvements. Importantly, we assessed both inpatient and outpatient lipid management, with interventions aimed at improving performance in both settings. Aubiniere-Robb et al. previously reported that a single interactive face-to-face teaching session, accompanied by illustrative reminders, improved early baseline lipid testing, with non-significant improvements in optimisation of LLTs, though in this case they only assessed whether patients were discharged on HIS.7 Salim et al. audited the prevalence of significantly elevated total cholesterol (≥7.2 mmol/L) in patients presenting with ACS, and reported that outpatient repeat measurement was only performed in 13% of these patients; they did not report whether any interventions were performed to improve performance.8
Our finding that local lipid assessment required updating is not unique: there is substantial variation in the performance of lipid testing across the UK.17 While quality improvement initiatives might drive local improvements, as reported here, national standardisation of lipid testing requires a top-down approach, the topic of a recent consensus statement.17 Additionally, integration of lipid reassessment and optimisation within secondary care pathways may drive further improvements in post-ACS lipid management. Jones reported the effects of a lipid-management pathway on improved lipid management after ACS.18 Although details were not fully reported, it was implied that a key change was to repeat lipid testing within four to six weeks post-ACS, embedded in the local cardiac rehabilitation programme, which may additionally help standardise post-ACS LLT management. We have considered similar interventions, but it is important to note that they are highly resource-intensive (e.g. for our centre, projected 400 in-area patients per year requiring follow-up blood tests within six weeks of admission, with potential further follow-up and optimisation), for which no supporting resources exist at present.
Integration of interventions within electronic health records will likely deliver more reliable, sustainable improvements. Such digitally based interventions might include prompts for lipid testing where patients are identified as having ACS, recommendations for drug escalation based on documented medical therapy and lipid results, and selectable, auto-populated discharge letter templates. One study reported that ‘electronic nudges’ (i.e. automated prompts) to clinicians resulted in increased statin prescriptions, though this was in the primary-care setting, predominantly for primary prevention;19 the post-ACS setting would potentially require more complicated prompts in those already established on LLT. Our trust, currently, does not utilise a single unified electronic patient record system, with separate systems for note documentation, bloods requesting, and electronic discharge letters. A unified electronic patient record is in the process of being implemented, which may help in improving compliance and ensuring more sustainable change, in particular with two of our observations: first, that the discharge template was only used in 22% of patients (related to the nature of our clinical systems: we were unable to introduce modifications to the discharge letter system, so clinicians had to access the template separately and copy it for use); second, that patients not directly admitted via the ED did not reliably undergo lipid testing on admission (potentially addressable by incorporating an ‘ACS bundle’ into an electronic patient management system).
Achieving therapeutic lipid control, and adjunctive agents
In our cohort, 65% of patients achieved NICE-defined absolute non-HDL-C targets at one year. This is similar to other reports in the literature: in the SWEDEHEART registry, the median non-HDL-C one-year post-ACS was 2.3 (1.9–2.9) mmol/L.20 Of note, the non-HDL-C target in NICE guidelines corresponds to a LDL-C of approximately 2.0 mmol/L, which contrasts with guidelines from the European Society of Cardiology (ESC) targeting a LDL-C of 1.4 mmol/L after ACS.21 In practice, this LDL-C target is rarely reached in national registries (20–33%),22,23 often due to a combination of non-adherence, therapy de-escalation, or therapeutic inertia (evidence suggests that LLT is rarely modified after discharge).
Adjunctive LLTs may lead to greater levels of therapeutic lipid modification. However, our data highlight an important issue, which, to our knowledge, has not been reported in the UK previously: that few patients are theoretically eligible for these agents, although in the context of partial re-testing of our cohort. Eligibility for inclisiran is not well-described; while there are descriptions of results for single-centre cohorts of patients prescribed inclisiran, these include patients with familial hypercholesterolaemia, and do not mention the overall number of patients screened.24 On the other hand, our report that approximately one-fifth of reassessed patients were eligible for IPE is similar to international reports: a large population cohort study in Canada suggested that 25% of patients with established atherosclerotic CV disease were eligible for IPE.25
Given the evidence suggests that even more intensive lipid lowering after ACS, beyond current guideline targets, may yield further benefits in secondary prevention, novel strategies of combination therapy, with early reassessment and uptitration, and less stringent thresholds for adjunctive LLTs, may be beneficial, though the associated practicalities and health economics will need to be explored and reviewed at a national level.26 The ORION-4 trial (NCT03705234) of inclisiran versus placebo in patients with established atherosclerotic CV disease, is due to report its findings in 2027, and may provide evidence for extending eligibility for patients with ACS.
Finally, while adjunctive LLTs (and other emerging therapies) provide promise for the future of LLT and CV risk modification, our data and others show that a significant implementation gap remains, with patients frequently not undergoing therapy escalation despite subtherapeutic lipid lowering.27 Such strategies might include altering the timing of testing and increased collaboration between primary and secondary care, and greater adoption of combination therapies, though these will need to be examined prospectively in larger studies.
Limitations
While we demonstrate marked improvements, further, ongoing improvements are required across the board. Although the absolute number of patients included was small, it represented nearly a quarter of yearly ACS admissions to our centre, and, therefore, is likely to be broadly representative of local trends in management and eligibility for adjunctive LLTs.
We only evaluated eligibility for adjunctive agents in cycle 2, as few patients in cycle 1 underwent complete lipid assessment after discharge. Despite improvements between cycles 1 and 2, a low proportion of LDL-C remeasurement in those patients with subtherapeutic non-HDL-C, means that we were only able to estimate the theoretical eligibility for inclisiran and IPE. The guidance for IPE eligibility requires fasting samples. Samples in our system are not routinely marked as fasting/non-fasting, and so our report of theoretical eligibility remains an estimate only: non-fasting samples are estimated to be associated with a mean maximal 0.3 mmol/L increase in triglyceride concentrations,28 and in those patients who were identified as theoretically eligible for IPE, two had triglyceride concentrations within 0.3 mmol/L of the cut-off.
We did not analyse eligibility for alirocumab and evolocumab, as the thresholds for use in patients with a single CV event without a diagnosis of familial hypercholesterolaemia (LDL-C >4.0 mmol/L), are higher than that for inclisiran. Eligibility rates are, therefore, known to be lower.8 Bempedoic acid is currently only recommended in combination with ezetimibe in statin-intolerant patients, although this information is not always clearly documented in linked community records.29
Conclusion
We demonstrate that our structured intervention to improve lipid management is associated with improvements in inpatient and outpatient lipid management. However, a third of patients fail to achieve therapeutic non-HDL-C lowering at one year. A proportion of these patients are theoretically eligible for adjunctive LLTs, but real-world use is lower than would be expected. Novel strategies to achieve therapeutic lipid lowering in this population are needed.
Key messages
- Lipid management is a key component of secondary prevention after acute coronary syndrome, but adherence to guidelines is generally poor
- Adjuncts to statin therapy are now available for clinical use, but applicability of agents, such as inclisiran and icosapent ethyl, in real-world secondary prevention populations in the UK is poorly characterised
- In this study, we present the results of a two-stage quality improvement project designed to improve lipid management in a district general hospital, demonstrating improvements in admission lipid assessment, lipid-lowering therapy management, discharge communications, and lipid reassessment
- Furthermore, we assessed the eligibility of patients for adjunctive lipid-lowering agents (ezetimibe, inclisiran and icosapent ethyl) after acute coronary syndrome
Conflicts of interest
None declared.
Funding
None.
Study approval
The project was registered and approved locally by the Clinical Audit and Effectiveness Department, Great Western Hospital (DOM-053/1, DOM-054/1).
References
1. World Health Organisation. Global health estimates: leading causes of death. Geneva: WHO, 2024. Available from: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates/ghe-leading-causes-of-death#:~:text=The%20world’s%20biggest%20killer%20is,9.0%20million%20deaths%20in%202021 [accessed June 2025].
2. Steen DL, Khan I, Andrade K et al. Event rates and risk factors for recurrent cardiovascular events and mortality in a contemporary post acute coronary syndrome population representing 239 234 patients during 2005 to 2018 in the United States. J Am Heart Assoc 2022;11:e022198. https://doi.org/10.1161/JAHA.121.022198
3. Ference BA, Ginsberg HN, Graham I et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur Heart J 2017;38:2459–72. https://doi.org/10.1093/eurheartj/ehx144
4. Collins R, Reith C, Emberson J et al. Interpretation of the evidence for the efficacy and safety of statin therapy. Lancet 2016;388:2532–61. https://doi.org/10.1016/S0140-6736(16)31357-5
5. National Institute for Health and Care Excellence. Cardiovascular disease: risk assessment and reduction, including lipid modification. CG181. London: NICE, 2014. Available from: https://www.nice.org.uk/guidance/CG181
6. National Institute for Health and Care Excellence. Cardiovascular disease: risk assessment and reduction, including lipid modification. NG238. London: NICE, 2023. Available from: https://www.nice.org.uk/guidance/ng238
7. Aubiniere-Robb L, Dickerson JE, Brady AJB. Lipid testing and treatment after acute myocardial infarction: no flags for the flagship. Br J Cardiol 2019;26:141–4. https://doi.org/10.5837/bjc.2019.041
8. Salim HY, Lwin K, Khoo C et al. Management of hyperlipidaemia following acute coronary syndrome: a retrospective audit. Br J Cardiol 2021;28:62–6. https://doi.org/10.5837/bjc.2021.017
9. National Institute for Health and Care Excellence. Acute coronary syndrome. NG185. London: NICE, 2020. Available from: https://www.nice.org.uk/guidance/ng185
10. Sabatine MS, Giugliano RP, Keech AC et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med 2017;376:1713–22. https://doi.org/10.1056/NEJMoa1615664
11. Schwartz GG, Steg GP, Szarek M et al. Alirocumab and cardiovascular outcomes after acute coronary syndrome. N Engl J Med 2018;379:2097–107. https://doi.org/10.1056/NEJMoa1801174
12. Ray KK, Wright RS, Kallend D et al. Two phase 3 trials of inclisiran in patients with elevated LDL cholesterol. N Engl J Med 2020;382:1507–19. https://doi.org/10.1056/NEJMoa1912387
13. Bays HE, Ballantyne CM, Braeckman RA, Stirtan WG, Soni PN. Icosapent ethyl, a pure ethyl ester of eicosapentaenoic acid: effects on circulating markers of inflammation from the MARINE and ANCHOR studies. Am J Cardiovasc Drugs 2013;13:37–46. https://doi.org/10.1007/s40256-012-0002-3
14. Bhatt DL, Steg GP, Miller M et al. Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridaemia. N Engl J Med 2019;380:11–22. https://doi.org/10.1056/NEJMoa1812792
15. National Institute for Health and Care Excellence. Inclisiran for treating primary hypercholesterolaemia or mixed dyslipidaemia. TA733. London: NICE, 2021. Available from: https://www.nice.org.uk/guidance/ta733
16. National Institute for Health and Care Excellence. Icosapent ethyl with statin therapy for reducing the risk of cardiovascular events in people with raised triglycerides. TA805. London: NICE, 2022. Available from: https://www.nice.org.uk/guidance/ta805
17. Kenkre JS, Mazaheri, Nely RDG et al. Standardising lipid testing and reporting in the United Kingdom; a joint statement by HEART UK and the Association for Laboratory Medicine. Ann Clin Biochem 2025;62:257–86. https://doi.org/10.1177/00045632251315303
18. Jones C. Evaluation of a lipid management pathway within a local cardiac rehabilitation service. Br J Cardiol 2022;29:137–40. https://doi.org/10.5837/bjc.2022.034
19. Adusumalli S, Kanter GP, Small DS et al. Effect of nudges to clinicians, patients, or both to increase statin prescribing: a cluster randomized clinical trial. JAMA Cardiol 2023;8:23–30. https://doi.org/10.1001/jamacardio.2022.4373
20. Schubert J, Leosdottir M, Lindahl B et al. Intensive early and sustained lowering of non-high-density lipoprotein cholesterol after myocardial infarction and prognosis: the SWEDEHEART registry. Eur Heart J 2024;39:4204–15. https://doi.org/10.1093/eurheartj/ehae576
21. Mach F, Koskinas KC, van Lennep JER et al. 2025 focused update of the 2019 ESC/EAS guidelines for the management of dyslipidaemias. Eur Heart J 2025;46:4359–78. https://doi.org/10.1093/eurheartj/ehaf190
22. De Backer G, Jankowski P, Kotseva K et al. Management of dyslipidaemia in patients with coronary heart disease: results from the ESC-EORP EUROASPIRE V survey in 27 countries. Atherosclerosis 2019;285:135–46. https://doi.org/10.1016/j.atherosclerosis.2019.03.014
23. Ray KK, Molemans B, Schoonen WM et al. EU wide cross-sectional observational study of lipid-modifying therapy use in secondary and primary care: the DA VINCI study. Eur J Prev Cardiol 2021;28:1279–89. https://doi.org/10.1093/eurjpc/zwaa047
24. Padam P, Barton L, Wilson S et al. Lipid lowering with inclisiran: a real-world single-centre experience. Open Heart 2022;9:e002184. https://doi.org/10.1136/openhrt-2022-002184
25. Lawler PR, Kotrri G, Koh M et al. Real-world risk of cardiovascular outcomes associated with hypertriglyceridaemia among individuals with atherosclerotic cardiovascular disease and potential eligibility for emerging therapies. Eur Heart J 2020;41:86–94. https://doi.org/10.1093/eurheartj/ehz767
26. Gargiulo P, Ray KK, Perrone-Filardi P. Combination lipid-lowering strategies after acute coronary syndrome: reconsidering cholesterol targets. Eur Heart J 2025;ehaf615. Online ahead of print. https://doi.org/10.1093/eurheartj/ehaf615
27. Zheutlin AR, Derington CG, Herrick JS et al. Lipid-lowering therapy use and intensification among United States veterans following myocardial infarction or coronary revascularization between 2015 and 2019. Circ Cardiovasc Qual Outcomes 2022;15:e008861. https://doi.org/10.1161/CIRCOUTCOMES.121.008861
28. Nordestgaard BG. A test in context: lipid profile, fasting versus nonfasting. J Am Coll Cardiol 2017;70:1637–46. https://doi.org/10.1016/j.jacc.2017.08.006
29. National Institute for Health and Care Excellence. Bempedoic acid with ezetimibe for treating primary hypercholesterolaemia or mixed dyslipidaemia. TA694. London: NICE, 2021. Available from: https://www.nice.org.uk/guidance/ta694
 Real-world efficacy of inclisiran: data from a tertiary lipid clinic
Real-world efficacy of inclisiran: data from a tertiary lipid clinic 