Severe gradient (mean >40 mmHg) and moderate area (EOA >1.0 cm2)
This can be caused by erroneous placement of the sub-aortic pulsed sample too far into the valve, so that the VTI1 component of the continuity equation is too high. It can also occur if the measurement of the LV outflow diameter is erroneously large or in the presence of high flow, for example with moderate aortic regurgitation, anaemia, or sepsis. A dagger- shaped CW signal (see figure 2) together with good mobility of one or more cusps suggests that EOA is the more representative measure.

The rest of the heart
Aortic regurgitation
This is graded according to established American Society of Echocardiography (ASE)/European Association of Echocardiography (EAE) guidelines2 (see below).
The right heart
Severe AS is associated with pulmonary hypertension and ultimately right ventricular failure. The risk of surgery is then substantially raised.6
The mitral valve
Functional mitral regurgitation may develop in severe AS as the LV starts to dilate. Mitral surgery is likely to be necessary if the mitral valve is anatomically abnormal (e.g. prolapsing), or the regurgitation is more than moderate. 7,8
The aorta
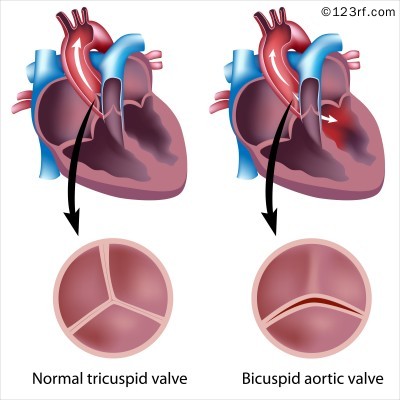
Aortic root dilatation and coarctation are associated with a bicuspid aortic valve (see figure 3).
Surgery may be indicated for aortic dilatation even if the AS remains symptom-free.
Exercise echocardiography may provide useful additional information in patients with asymptomatic severe AS. During exercise, the development of symptoms attributable to AS, a fall in blood pressure below baseline or an increase in mean gradient of >20 mmHg, are associated with an adverse outcome and may warrant consideration of valve surgery in individual cases.9
Advanced echo techniques
Transoesophageal echocardiography and 3D
3D echocardiography can allow planimetry of the LV outflow tract in the calculation of the effective orifice area.10 Before transcatheter aortic valve implantation (TAVI) it gives a better assessment of aortic annulus size than on 2D to allow preparation of the TAVI valve.
Transoesophageal echocardiography (TOE) is occasionally used to measure the geometric orifice area by planimetry but this is at best a semi-quantitative measure owing to the irregular 3D configuration of the orifice. However, it is useful for the assessment immediately before TAVI, particularly for measuring the annulus diameter. It is also useful during and after the procedure for the detection of complications.11
Stress echocardiography
Low-dose dobutamine stress echocardiography is used in low-flow, low gradient AS particularly if the EF is low. It can differentiate whether: i) the impairment of LV systolic function has been caused by severe AS or; ii) whether the reduction of LV systolic function gives the appearance of severe AS by reduced valve leaflet opening. The study has two aims:
- is there contractile reserve (increase in VTI, EF or flow by >20%)
- is the AS severe (mean gradient >30 mmHg at any point during the test).6,12–13
Stress echocardiography is also useful if the patient has symptoms despite unequivocally moderate AS. This is to:
- reveal LV wall motion abnormalities as a result of coexistent coronary disease
- test the compliance of the aortic valve. Severe stenosis is usually taken as a rise of >20 mmHg during stress.
There is an argument for performing exercise stress echocardiography in all patients with asymptomatic severe AS, looking for possible indications for surgery or high risk features suggesting that a cardiac event may occur with an one year:
- revealed symptoms
- a blunted blood pressure rise (by less than 20 mmHg)
- failure of the EF to increase during exercise
- increase in mean gradient by >20 mmHg with a resting mean gradient >35 mmHg.14
