The tricuspid valve
Minimum echocardiographic dataset
The minimum echocardiographic dataset for the tricuspid valve consists of:
- a detailed description of the appearance and motion of the valve
- colour map width
- diastolic V max, mean gradient and pressure half-time if there is stenosis
- tricuspid annulus diameter
- RV size and systolic function
- pulmonary artery pressure
- presence of left-sided disease.
Grading tricuspid valve disease (see table 7)
Colour jet
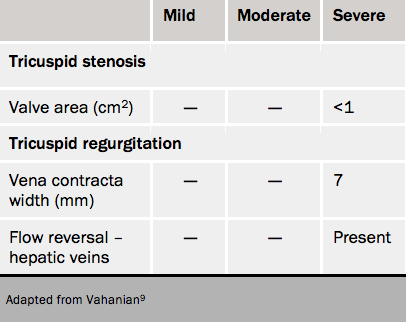
Tricuspid regurgitation is graded by the width of the vena contracta of the systolic colour signal in multiple views. A width ≥7 mm is indicative of severe regurgitation although there are no well validated cut-offs for differentiating mild from moderate tricuspid regurgitation.32
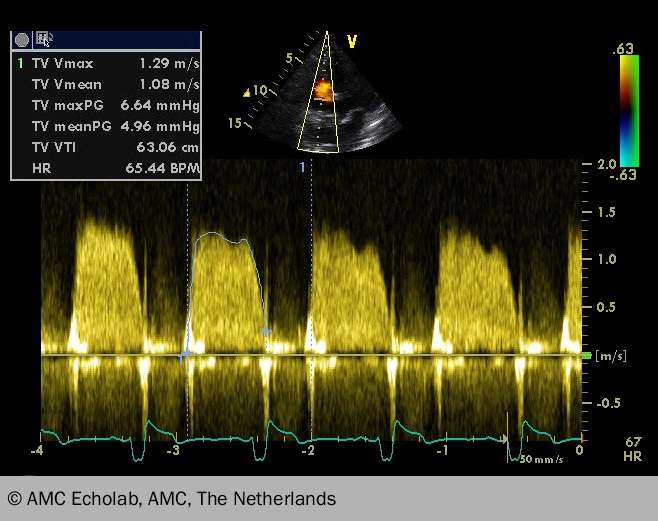
CW signal
In severe regurgitation, the signal is intense and triangular in shape. The jet is a useful means for assessing the tricuspid regurgitation (TR) severity. With more mild regurgitation the spectral Doppler signal is less intense than forward flow and may not be complete. In that it resembles a CW transaortic signal. On CW Doppler across the tricuspid valve, a mean gradient of ≥5 mmHg is taken to be severe along with a pressure T1/2 ≥190 ms
Hepatic vein
Where possible, a pulsed wave (PW) Doppler trace should be obtained within the hepatic vein, looking for systolic flow reversal (80% sensitivity for severe TR).44 In addition to an assessment of TR severity its haemodynamic consequences should also be evaluated.
The rest of the heart
Right ventricle
In severe compensated TR, the RV may be normal in size but demonstrate dynamic systolic function. With chronicity, the RV may progressively dilate (see figure 14) and demonstrate impaired systolic function, whilst the right atrium dilates and the interatrial septum bows towards the left, reflecting elevated right atrial pressure. A tricuspid annulus excursion of <15 mm is a sensitive indicator of impaired right ventricular function whilst an RV systolic maximum tissue Doppler velocity at the base of the RV free wall of <11 cm/s indicates a RV ejection fraction (RVEF) <45%.45
In severe tricuspid stenosis (see figure 15), the leaflets will be calcified or restricted and demonstrate limited mobility, and a valve area ≤1cm2 by the continuity equation. Other surrogate measures of significant tricuspid stenosis include a dilated right atrium and inferior vena cava reflecting elevated right atrial pressures.
Cardiac computed tomography in tricuspid valve disease
CT is not useful. The stenosed tricuspid valve may appear thickened, calcified or shortened. In tricuspid regurgitation, malcoaption may occasionally be imaged. Secondary effects of tricuspid stenosis include right atrial dilatation, dilatation of the inferior vena cava (IVC) and superior vena cava (SVC) and reflux of contrast into the hepatic veins.
Cardiac magnetic resonance imaging
In tricuspid stenosis (TS), turbulent flow may be seen across the tricuspid valve with in-plane SSFP imaging. Although it is technically feasible to measure the peak velocity across the tricuspid valve, this is not often used in clinical practice.
Tricuspid regurgitation may be seen as a black signal void with cine imaging. Regurgitant volumes and fraction can be calculated by measuring the forward stroke volume in the main pulmonary artery and subtracting this from the RV stroke volume on SSFP imaging, although this is not used clinically.
