The pulmonary valve
Minimum echocardiographic dataset
The minimum echocardiographic dataset for the pulmonary valve consists of:24
- appearance of the valve
- colour map – in severe regurgitation reversed flow fills the whole pulmonary artery lumen to the branches and beyond and the jet within the RV is broad
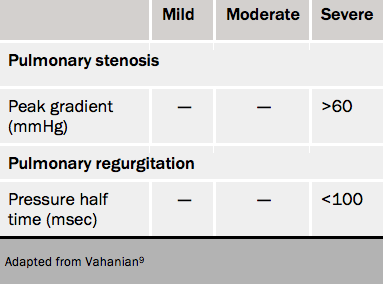
- spectral Doppler for systolic V max and regurgitant pressure half (typically <100 ms in severe pulmonary regurgitation [PR])
- effect on right ventricle
- pulmonary artery size
- pulmonary artery pressure which may drive the regurgitation.
Grading pulmonary valve disease
This is summarised in table 8.
Cardiac computed tomography in pulmonary disease
Since pulmonary stenosis is usually congenital in origin, cardiac CT may be useful in defining complex congenital heart anatomy. In patients with pulmonary stenosis, the leaflets are often thin and difficult to visualise directly and so surrogate markers of pulmonary stenosis are usually required. These include dilatation of the main pulmonary artery and left pulmonary artery, right ventricular hypertrophy, right atrial enlargement and bowing of the interatrial septum to the left in keeping with elevated right atrial pressures.
Cardiac CT is of limited use in evaluating PR and is confined to the detection of secondary effects such as dilatation of the pulmonary valve annulus, pulmonary artery dilatation and right ventricular dilatation.
Cardiac magnetic resonance imaging
Turbulent flow in pulmonary stenosis can be visualised with SSFP cine imaging. Although planimetry of the pulmonary valve is of limited use, as with the aortic valve, CMR is able to provide accurate peak velocity data across the aortic valve.
CMR is the gold standard for the assessment of PR.46 With visualisation of PR using cine SSFP imaging and the ability to accurately measure regurgitant volumes and regurgitant fractions with flow imaging, it has now become the technique of choice for the serial evaluation of patients with congenital heart disease, where progressive RV dilatation and RV dysfunction are important for the timing of pulmonary valve intervention.
Key learning messages
- Echocardiography is the mainstay of investigation
- CT and CMR are useful for the assessment of the aorta e.g. bicuspid aortic valve disease
- CT is useful in the work-up towards TAVI
- An ideal evaluation of a valvular lesion should include a description as to the aetiology of the valvular lesion, a qualitative and quantitative assessment of severity, an assessment of the haemodynamic effects on chamber size and function, and also an evaluation of concomitant valvular disease.
close window and return to take test
References
1. Nishimura RA, Otto CM, Bonow RO, et al. AHA/ACC Guideline for the management of patients with valvular heart disease. J Am Coll Cardiol 2014;63:e57–185. http://dx.doi.org/10.1016/j.jacc.2014.02.536
2. Baumgartner H, Hung J, Bermejo J, et al. Echocardiographic assessment of valve stenosis: EAE/ASE recommendations for clinical practice. Eur J Echocardiogr 2009;10:1–25. http://dx.doi.org/10.1093/ejechocard/jen303
3. Otto CM, Pearlman AS, Comess KA, Reamer RP, Janko CL, Huntsman LL. Determination of the stenotic aortic valve area in adults using Doppler echocardiography. J Am Coll Cardiol 1986;7:509–17. http://dx.doi.org/10.1016/S0735-1097(86)80460-0
4. Zoghbi WA, Farmer KL, Soto JG, Nelson JG, Quinones MA. Accurate noninvasive quantification of stenotic aortic valve area by Doppler echocardiography. Circulation 1986;73:452–9. http://dx.doi.org/10.1161/01.CIR.73.3.452
5. Chambers J. Low “gradient”, low flow aortic stenosis. Heart 2006;92:554–8. http://dx.doi.org/10.1136/hrt.2005.079038
6. Monin JL, Quere JP, Monchi M, et al. Low-gradient aortic stenosis: operative risk stratification and predictors for long-term outcome: a multicenter study using dobutamine stress hemodynamics. Circulation 2003;108:319–24. http://dx.doi.org/10.1161/01.CIR.0000079171.43055.46
7. Wan CK, Suri RM, Li Z, et al. Management of moderate functional mitral regurgitation at the time of aortic valve replacement: is concomitant mitral valve repair necessary? J Thorac Cardiovasc Surg 2009;137:635–40. http://dx.doi.org/10.1016/j.jtcvs.2008.11.015
8. Unger P, Dedobbeleer C, Van Camp G, Plein D, Cosyns B, Lancellotti P. Mitral regurgitation in patients with aortic stenosis undergoing valve replacement. Heart 2010;96:9–14. http://dx.doi.org/10.1136/hrt.2009.165548
9. Vahanian A, Alfieri O, Andreotti F, et al. Guidelines on the management of valvular heart disease (version 2012): The Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Euro Heart J 2012;33:2451–96. http://dx.doi.org/10.1093/eurheartj/ehs109/
10. Gutierrez-Chico JL, Zamorano JL, Prieto-Moriche E, et al. Real-time three-dimensional echocardiography in aortic stenosis: a novel, simple, and reliable method to improve accuracy in area calculation. Eur Heart J 2008;29:1296–306. http://dx.doi.org/10.1093/eurheartj/ehm467
11. Rajani R, Hancock J, Chambers J. Imaging: the art of TAVI. Heart 2012;98 (Suppl 4): iv14–iv22.
12. Nishimura RA, Grantham JA, Connolly HM, Schaff HV, Higano ST, Holmes DR, Jr. Low-output, low-gradient aortic stenosis in patients with depressed left ventricular systolic function: the clinical utility of the dobutamine challenge in the catheterization laboratory. Circulation 2002;106:809–13. http://dx.doi.org/10.1161/01.CIR.0000025611.21140.34
13. Takeda S, Rimington H, Chambers J. The relation between transaortic pressure difference and flow during dobutamine stress echocardiography in patients with aortic stenosis. Heart 1999;82:11–4. http://dx.doi.org/10.1136/hrt.82.1.11
14. Marechaux S, Hachicha Z, Bellouin A, et al. Usefulness of exercise-stress echocardiography for risk stratification of true asymptomatic patients with aortic valve stenosis. Eur Heart J 2010;31:1390–7. http://dx.doi.org/10.1093/eurheartj/ehq076
15. Shah RG, Novaro GM, Blandon RJ, Whiteman MS, Asher CR, Kirsch J. Aortic valve area: meta-analysis of diagnostic performance of multi-detector computed tomography for aortic valve area measurements as compared to transthoracic echocardiography. Int J Cardiovasc Imaging 2009;25:601–9. http://dx.doi.org/10.1007/s10554-009-9464-z
16. Willson AB, Webb JG, Labounty TM, et al. 3-dimensional aortic annular assessment by multidetector computed tomography predicts moderate or severe paravalvular regurgitation after transcatheter aortic valve replacement: a multicenter retrospective analysis. J Am Coll Cardiol 2012;59:1287–94. http://dx.doi.org/10.1016/j.jacc.2011.12.015
17. Jilaihawi H, Kashif M, Fontana G, et al. Cross-sectional computed tomographic assessment improves accuracy of aortic annular sizing for transcatheter aortic valve replacement and reduces the incidence of paravalvular aortic regurgitation. J Am Coll Cardiol 2012;59:1275–86. http://dx.doi.org/10.1016/j.jacc.2011.11.045
18. Clavel MA, Pibarot P, Messika-Zeitoun D, et al. Impact of aortic valve calcification, as measured by MDCT, on survival in patients with aortic stenosis. Results of an international registry study. J Am Coll Cardiol 2014;64:1202–13. http://dx.doi.org/10.1016/j.jacc.2014.05.066
19. Kamperidis V, van Rosendael PJ, Katsanos S, et al. Low gradient severe aortic stenosis with preserved ejection fraction: reclassification of severity by fusion of Doppler and computed tomographic data. Euro Heart J 2015;36:2087–96. http://dx.doi.org/10.1093/eurheartj/ehv188
20. Koos R, Kuhl HP, Muhlenbruch G, Wildberger JE, Gunther RW, Mahnken AH. Prevalence and clinical importance of aortic valve calcification detected incidentally on CT scans: comparison with echocardiography. Radiology 2006;241:76–82. http://dx.doi.org/10.1148/radiol.2411051163
21. Debl K, Djavidani B, Seitz J, et al. Planimetry of aortic valve area in aortic stenosis by magnetic resonance imaging. Investigative radiology 2005;40:631–6. http://dx.doi.org/10.1097/01.rli.0000178362.67085.fd
22. Caruthers SD, Lin SJ, Brown P, et al. Practical value of cardiac magnetic resonance imaging for clinical quantification of aortic valve stenosis: comparison with echocardiography. Circulation 2003;108:2236–43. http://dx.doi.org/10.1161/01.CIR.0000095268.47282.A1
23. Dweck MR, Joshi S, Murigu T, et al. Midwall fibrosis is an independent predictor of mortality in patients with aortic stenosis. J Am Coll Cardiol 2011;58:1271–9. http://dx.doi.org/10.1016/j.jacc.2011.03.064
24. Lancellotti P, Tribouilloy C, Hagendorff A, et al. European Association of Echocardiography recommendations for the assessment of valvular regurgitation. Part 1: aortic and pulmonary regurgitation (native valve disease). Eur J Echocardiogr 2010;11:223–44. http://dx.doi.org/10.1093/ejechocard/jeq030
25. Griffin BP, Flachskampf FA, Siu S, Weyman AE, Thomas JD. The effects of regurgitant orifice size, chamber compliance, and systemic vascular resistance on aortic regurgitant velocity slope and pressure half-time. Am Heart J 1991;122:1049–56. http://dx.doi.org/10.1016/0002-8703(91)90471-S
26. Tribouilloy C, Avinee P, Shen WF, Rey JL, Slama M, Lesbre JP. End diastolic flow velocity just beneath the aortic isthmus assessed by pulsed Doppler echocardiography: a new predictor of the aortic regurgitant fraction. Br Heart J 1991;65:37–40. http://dx.doi.org/10.1136/hrt.65.1.37
27. Detaint D, Messika-Zeitoun D, Maalouf J, et al. Quantitative echocardiographic determinants of clinical outcome in asymptomatic patients with aortic regurgitation: a prospective study. JACC: Cardiovascular Imaging 2008;1:1–11. http://dx.doi.org/10.1016/j.jcmg.2007.10.008
28. Feuchtner GM, Dichtl W, Schachner T, et al. Diagnostic performance of MDCT for detecting aortic valve regurgitation. Am J Roentgenol 2006;186:1676–81. http://dx.doi.org/10.2214/AJR.05.0967
29. Myerson SG. Heart valve disease: investigation by cardiovascular magnetic resonance. J Cardiovasc Magn Reson 2012;14:7. http://dx.doi.org/10.1186/1532-429X-14-7
30. Honda N, Machida K, Hashimoto M, et al. Aortic regurgitation: quantitation with MR imaging velocity mapping. Radiology 1993;186:189–94. http://dx.doi.org/10.1148/radiology.186.1.8416562
31. Myerson SG, d’Arcy J, Mohiaddin R, et al. Aortic regurgitation quantification using cardiovascular magnetic resonance. Association with clinical outcome. Circulation 2012;126:1452-6. http://dx.doi.org/10.1161/CIRCULATIONAHA.111.083600
32. Lancellotti P, Moura L, Pierard LA, et al. European Association of Echocardiography recommendations for the assessment of valvular regurgitation. Part 2: mitral and tricuspid regurgitation (native valve disease). Eur J Echocardiogr 2010;11:307–32. http://dx.doi.org/10.1093/ejechocard/jeq031
33. Tribouilloy C, Shen WF, Rey JL, Adam MC, Lesbre JP. Mitral to aortic velocity-time integral ratio. A non-geometric pulsed-Doppler regurgitant index in isolated pure mitral regurgitation. Euro Heart J 1994;15:1335–9.
34. Garbi M, Chambers J, Vannan MA, Lancellotti P. Valve stress echocardiography: a practical guide for referral, procedure, reporting and clinical implementation of results. On behalf of the HAVEC group. JACC Imaging 2015;8:724–36. http://dx.doi.org/10.1016/j.jcmg.2015.02.010
35. Lancellotti P, Troisfontaines P, Toussaunt AC, Pierard LA. Prognostic importance of exercise-induced changes in mitral regurgitation in patients with chronic ischaemic left ventricular dysfunction. Circulation 2003;108:1713–7. http://dx.doi.org/10.1161/01.CIR.0000087599.49332.05
36. Alkadhi H, Wildermuth S, Bettex DA, et al. Mitral regurgitation: quantification with 16-detector row CT–initial experience. Radiology 2006;238:454–63. http://dx.doi.org/10.1148/radiol.2381042216
37. Chan KM, Wage R, Symmonds K, et al. Towards comprehensive assessment of mitral regurgitation using cardiovascular magnetic resonance. J Cardiovasc Magn Reson 2008;10:61. http://dx.doi.org/10.1186/1532-429X-10-61
38. Wilkins GT, Weyman AE, Abascal VM, Block PC, Palacios IF. Percutaneous balloon dilatation of the mitral valve: an analysis of echocardiographic variables related to outcome and the mechanism of dilatation. Br Heart J 1988;60:299–308. http://dx.doi.org/10.1136/hrt.60.4.299
39. Zamorano J, Cordeiro P, Sugeng L, et al. Real-time three-dimensional echocardiography for rheumatic mitral valve stenosis evaluation. J Am Coll Cardiol 2004;43:2091–6. http://dx.doi.org/10.1016/j.jacc.2004.01.046
40. Thomas JD, Weyman AE. Doppler mitral pressure half-time: a clinical tool in search of theoretical justification. J Am Coll Cardiol 1987;10:923–9. http://dx.doi.org/10.1016/S0735-1097(87)80290-5
41. Messika-Zeitoun D, Serfaty JM, Laissy JP, et al. Assessment of the mitral valve area in patients with mitral stenosis by multislice computed tomography. J Am Coll Cardiol 2006;48:411–3. http://dx.doi.org/10.1016/j.jacc.2006.04.035
42. Djavidani B, Debl K, Lenhart M, et al. Planimetry of mitral valve stenosis by magnetic resonance imaging. J Am Coll Cardiol 2005;45:2048–53. http://dx.doi.org/10.1016/j.jacc.2005.03.036
43. Djavidani B, Debl K, Buchner S, et al. MRI planimetry for diagnosis and follow-up of valve area in mitral stenosis treated with valvuloplasty. RoFo 2006;178:781–6. http://dx.doi.org/10.1055/s-2006-926876
44. Gonzalez-Vilchez F, Zarauza J, Vazquez de Prada JA, et al. Assessment of tricuspid regurgitation by Doppler color flow imaging: angiographic correlation. Int J Cardiol 1994;44:275–83. http://dx.doi.org/10.1016/0167-5273(94)90292-5
45. Haddad F, Doyle R, Murphy DJ, Hunt SA. Right ventricular function in cardiovascular disease, part II: pathophysiology, clinical importance, and management of right ventricular failure. Circulation 2008;117:1717–31. http://dx.doi.org/10.1161/CIRCULATIONAHA.107.653584
46. Baumgartner H, Bonhoeffer P, De Groot NMS, et al. ESC guidelines for the management of grown-up congenital heart disease (new version 2010). Euro Heart J 2010;31:2915–57. http://dx.doi.org/10.1093/eurheartj/ehq249
Recommended reading
Aronow WS, Schwartz KS, Koenigsberg M. Correlation of serum lipids, calcium and phosphorus, diabetes mellitus, aortic valve stenosis and history of systemic hypertension with presence or absence of mitral anular calcium in persons older than 62 years in a long-term health care facility. Am J Cardiol 1987;59:381–2. http://dx.doi.org/10.1016/0002-9149(87)90827-7
Antonini-Canterin F, Huang G, Cervesato E, et al. Symptomatic aortic stenosis: does systemic hypertension play an additional role? Hypertension 2003;41:1268–72. http://dx.doi.org/10.1161/01.HYP.0000070029.30058.59
Kadem L, Dumesnil JG, Rieu R, Durand LG, Garcia D, Pibarot P. Impact of systemic hypertension on the assessment of aortic stenosis. Heart 2005;91:354–61. http://dx.doi.org/10.1136/hrt.2003.030601
Garcia D, Pibarot P, Dumesnil JG, Sakr F, Durand LG. Assessment of aortic valve stenosis severity: A new index based on the energy loss concept. Circulation 2000;101:765–71. http://dx.doi.org/10.1161/01.CIR.101.7.765
Briand M, Dumesnil JG, Kadem L, et al. Reduced systemic arterial compliance impacts significantly on left ventricular afterload and function in aortic stenosis: implications for diagnosis and treatment. J Am Coll Cardiol 2005;46:291–8. http://dx.doi.org/10.1016/j.jacc.2004.10.081
Lancellotti P, Donal E, Magne J, et al. Risk stratification in asymptomatic moderate to severe aortic stenosis: the importance of the valvular, arterial and ventricular interplay. Heart 2010;96:1364–71. http://dx.doi.org/10.1136/hrt.2009.190942
Hachicha Z, Dumesnil JG, Bogaty P, Pibarot P. Paradoxical low-flow, low-gradient severe aortic stenosis despite preserved ejection fraction is associated with higher afterload and reduced survival. Circulation 2007;115:2856–64. http://dx.doi.org/10.1161/CIRCULATIONAHA.106.668681
Konen E, Goitein O, Feinberg MS, et al. The role of ECG-gated MDCT in the evaluation of aortic and mitral mechanical valves: initial experience. Am J Roentgenol 2008;191:26–31. http://dx.doi.org/10.2214/AJR.07.2951
Wilkins GT, Weyman AE, Abascal VM, Block PC, Palacios IF. Percutaneous balloon dilatation of the mitral valve: an analysis of echocardiographic variables related to outcome and the mechanism of dilatation. Br Heart J 1988;60:299–308. http://dx.doi.org/10.1136/hrt.60.4.299
Kon MW, Myerson SG, Moat NE, Pennell DJ. Quantification of regurgitant fraction in mitral regurgitation by cardiovascular magnetic resonance: comparison of techniques. J Heart Valve Dis 2004;13:600–7.
Kizilbash AM, Hundley WG, Willett DL, Franco F, Peshock RM, Grayburn PA. Comparison of quantitative Doppler with magnetic resonance imaging for assessment of the severity of mitral regurgitation. Am J Cardiol 1998;81:792–5. http://dx.doi.org/10.1016/S0002-9149(97)01024-2
close window and return to take test
All rights reserved. No part of this programme may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without the prior permission of the publishers, Medinews (Cardiology) Limited.
It shall not, by way of trade or otherwise, be lent, re-sold, hired or otherwise circulated without the publisher’s prior consent.
Medical knowledge is constantly changing. As new information becomes available, changes in treatment, procedures, equipment and the use of drugs becomes necessary. The editors/authors/contributors and the publishers have taken care to ensure that the information given in this text is accurate and up to date. Readers are strongly advised to confirm that the information, especially with regard to drug usage, complies with the latest legislation and standards of practice.
Healthcare professionals should consult up-to-date Prescribing Information and the full Summary of Product Characteristics available from the manufacturers before prescribing any product. Medinews (Cardiology) Limited cannot accept responsibility for any errors in prescribing which may occur.
