Low-density lipoprotein-cholesterol (LDL-C) is accepted as a causal risk factor for development of atherosclerotic cardiovascular disease (CVD) and acute coronary syndromes (ACS). In individuals aged 40–75 years, reducing LDL-C constitutes a main treatment target for prevention of atherosclerotic CVD in all international guidelines. Furthermore, diabetes mellitus (DM) confers a two-fold excess risk of vascular outcomes (coronary heart disease, ischaemic stroke, and vascular deaths), independent of other risk factors. Our audit project identified a deficit in current standards following an audit of adherence to lipid profile and glycated haemoglobin (HbA1c) testing in the high-risk chest pain population in our city hospital setting. We found only 49% of patients had LDL-C checked during their inpatient stay, and only 45% had HbA1c checked, of our targeted 100% of patients. This allowed the introduction of a planned intervention to improve admission testing and re-auditing demonstrated an improvement in testing, mainly driven by improved LDL-C testing. Despite this, a deficit still exists and more work is needed to meet our target of 100% compliance.
Introduction
Low-density lipoprotein-cholesterol (LDL-C) is accepted as a causal risk factor for development of atherosclerotic cardiovascular disease (CVD) and acute coronary syndromes (ACS).1 European Society of Cardiology (ESC) guidelines have been extensive in setting up lipid targets for primary and secondary prevention of CVD.2 The 2021 ESC guidelines carry forward the 2019 ESC dyslipidaemia targets to introduce a therapeutic regimen that achieves a ≥50% LDL-C reduction from baseline and a LDL-C goal of <1.4 mmol/L (<55 mg/dL) (very-high-risk group) or <1.8 mmol/L (high-risk group).2
The updated National Institute for Health and Care Excellence (NICE) guideline recommends starting high-dose statins as first line for secondary prevention of CVD, with an aim to achieve a greater than 40% reduction in non-high-density lipoprotein-cholesterol (non-HDL-C) levels.3 Reduction of 1 mmol/L in LDL-C was associated with a 12% proportional risk reduction in major vascular events after one year of treatment, 20% after three years of treatment, 23% after five years of treatment, and a 29% proportional risk reduction after seven years of treatment.4 Recently, newer classes of lipid-lowering drugs have been developed, which are now available in clinical practice. A summary of currently available lipid-lowering therapies is outlined in table 1, all of which have been demonstrated to have cardiovascular (CV) risk benefit.
Table 1. Evidence for current lipid-lowering therapies
| Medication | Mechanism of action | Evidence base |
| Statins | Competitive inhibitor of HMG-CoA reductase, the rate limiting enzyme responsible for cholesterol synthesis in the liver | Significant reduction in LDL-C and CV risk across many studies, with high-intensity statins showing a more significant lowering in LDL-C and CV risk16 Across all 26 trials, all-cause mortality was reduced by 10% per 1.0 mmol/L LDL-C reduction |
| Ezetimibe | Inhibits intestinal receptor responsible for cholesterol and phytosterol absorption | IMPROVE-IT demonstrated a significant reduction in CV risk when used in addition to simvastatin following ACS recovery. High-risk patients showed a 6.3% absolute risk reduction in CV death/MI/CVA at 7 years17 |
| PCSK9 inhibitors (inclisiran, alirocumab and evolocumab) | Inhibits PCSK9 activity, blocking LDL-receptor breakdown and lowering plasma LDL-C levels | 45% to 60% reduction in LDL-C when used alone or in combination with statins18,19 Alirocumab and evolocumab both demonstrate a significant relative risk reduction of 15% for CV events18,19 |
| Bempedoic acid | Reduces LDL-C by inhibiting ATP-citrate lyase, an enzyme in the cholesterol biosynthesis pathway | Decreases LDL-C by approximately 18% in patients who are on maximally tolerated statin therapy20 Also found to decrease LDL-C by 21% when used alone and by 28% when used in combination with ezetimibe20 The CLEAR trial demonstrated treatment with bempedoic acid among statin-intolerant patients was associated with a lower risk of major adverse cardiovascular events21 |
| Icosapent ethyl | Stable ethyl ester of EPA (omega-3 fatty acid) Reduces hepatic VLDL-TG synthesis and enhances triglyceride clearance | 25% reduction in CV risk over 5-year period demonstrated in REDUCE-IT trial22 Currently indicated in patients with very high triglycerides (>150 mg/dL) |
| Key: ACS = acute coronary syndrome; ATP = adenosine triphosphate; CV = cardiovascular; CVA = cerebrovascular accident; EPA = eicosapentaenoic acid; HMG-CoA = 3-hydroxy-3-methylglutaryl coenzyme A; LDL = low-density lipoprotein; LDL-C = low-density lipoprotein-cholesterol; MI = myocardial infarction; PCSK9 = proprotein convertase subtilisin/kexin type 9; VLDL-TG = very-low-density lipoprotein–triglyceride | ||
The latest NICE and ESC guidelines recommend that a lipid profile should be obtained for all patients presenting with ACS. ESC recommends a follow-up lipid profile four to six weeks after the start of treatment,2 whereas NICE recommends a repeat lipid sample three months after the start of therapy.3 There are variations in lipoprotein levels after acute myocardial infarction that manifest within 24 to 48 hours after the onset of chest pain, these levels are stabilised after two months.5
Diabetes mellitus (DM) confers a two-fold excess risk of vascular outcomes (coronary heart disease, ischaemic stroke, and vascular deaths), independent of other risk factors.6 In addition, diabetic patients with ACS suffer from increased mortality compared with non-diabetic patients.7 Hyperglycaemia is associated with impaired microvascular function and decreased coronary flow velocity and may induce microvascular obstruction in ACS patients. Diabetes increases atherosclerotic plaque formation and thrombosis, thereby contributing to myocardial infarction (MI).8 Hyperglycaemia and newly diagnosed DM are found in a large number of ACS patients and are a strong predictor for poor prognosis in these patients.9 Fasting and random glucose levels remain the most common test for diabetes mellitus, however, HbA1c level was shown to be a better predictor of prognosis following ACS than fasting and admission glucose.10 HbA1c has been identified as an independent predictor of mortality,11 and reflects average blood glucose concentrations over the previous 8–12 weeks. Admission level HbA1c is a predictor of mortality and major adverse events in patients with both ST-elevation and non-ST-elevation MI.10
A systematic review of 25 studies involving 304,253 ACS patients showed that elevated HbA1c is a predictor of in-hospital mortality in ACS patients and short-term mortality in ACS patients, regardless of pre-admission diabetic status.12 The latest NICE guidelines recommend that HbA1c should be tested in all patients with hyperglycaemia after ACS.13 Updated 2023 ESC guidelines discuss the management of CVD in patients with diabetes. Recognition and adequate treatment of DM, in turn, reduces risk of CV events. Lowering HbA1c to <53 mmol was proven to reduce long-term macrovascular events in a meta-analysis of over 27,000 patients.14 The relatively new sodium-glucose cotransporter-2 inhibitors (SGLT2i) have demonstrated a significant risk reduction in CV events across multiple studies of patients with and without diabetes mellitus, and have become the recommended glycaemic therapy for those with type 2 diabetes (T2DM) and CVD.14 These medications also slow progression of microvascular complications of DM, such as albuminuria and chronic kidney disease (CKD). As such, 2023 ESC guidelines give a class 1A recommendation to use of SGLT2i in those with T2DM and heart failure or CKD. Glucagon-like peptide-1 (GLP-1) receptor agonists are currently second-line treatments for diabetes and have demonstrated significant reduction in body weight and CV risk when used in diabetic patients. Specific ESC guidance has been given to consider GLP-1 receptor agonists in the management of those with T2DM with obesity to reduce CV risk.14
Aim
Our study collected data on LDL-C and HbA1c testing in the ‘high-risk’ chest pain population at the Glasgow Royal Infirmary between January and June 2023. We aimed to ascertain if all high-risk patients with chest pain are screened for diabetes and dyslipidaemia at our site.
As a cardiology centre involved in lipid research, 100% of patients should have LDL-C and HbA1c checked to guide treatment for primary or secondary prevention. We also aimed to determine at what point during admission screening is done, and improve testing at first presentation.
Background
Despite current ESC guidelines primarily using LDL-C targets, the initial blood order set for chest pain presentations for emergency department (ED) and acute assessment unit (AAU) included only a ‘partial lipid profile’ (consisting of total cholesterol and triglycerides, with no LDL-C). A glucose test was included in the initial order set, but no HbA1c. We hypothesised that this may be leading to suboptimal testing of LDL-C and HbA1c. Following the first cycle of data collection, the blood order set was updated to include a full lipid profile and HbA1c for all patients presenting with chest pain. Departmental teaching was delivered to cardiology, AAU and ED colleagues to inform them of the change and encourage use of the order set. Email correspondence was also cascaded to all staff in these sites to inform them of the new order set and give background about our project. A second round of data collection was completed in June 2023 following this intervention. Outcomes from the project were presented in poster format at the Scottish Cardiac Society Autumn meeting.
A previous study of lipid testing at our site in 2018 found only 50% of patients presenting with ACS had lipid testing of any kind throughout their admission.15 Our initial data demonstrate an improvement from this data cycle, with only 13% of our initial cohort receiving no lipid testing at any point in their admission. However, despite improvements throughout our study, we are still short of our 100% compliance target. As evidenced above, there are a number of effective lipid-lowering therapies at our disposal. To best utilise these therapies, however, we need to improve lipid testing standards at our site. The same is true for glycaemic control measures; how can we prevent CV complications if we do not establish diabetic status in our high-risk patients? Improving testing at the point of admission using our intervention allows prompt primary and secondary prevention measures to be implemented.
Method
The site for this study is the Glasgow Royal Infirmary, a major cardiology receiving centre with inpatient cardiology admission wards and coronary care unit (CCU). Inclusion criteria allowed any patient with a presenting complaint of chest pain who had been subsequently accepted and transferred to the cardiology department. Patients admitted from cardiology clinics or direct admissions were excluded, as part of the aim of the project was to audit lipid and HbA1c testing at the point of emergency admission to hospital. We audited all patients with high-risk chest pain, but collected data to delineate which were ultimately diagnosed with type 1 myocardial infarction (T1MI).
Biochemical results, case notes and online clinical portal systems were used to retrospectively collect data on the cycle 1 patient cohort. Lipid profile and HbA1c testing was audited at point of transfer to cardiology from the ED or AAU. Testing was again audited pre-discharge, to assess whether lipid profiles were tested at first assessment or at a later stage of cardiology admission. Following our intervention, a second round of data was collected from the cycle 2 cohort. Other data collected included: whether patients who presented already had a diagnosis of type 1 or 2 DM; whether they were diagnosed with a T1MI; any primary or secondary prevention medications they were on pre-admission. This allows further context to be drawn from results of lipid and HbA1c testing. The numerical values of patient’s HbA1c and components of lipid testing were also collected, where available. As an audit of routinely collected clinical data, this study did not require an ethics proposal.
Table 2. Patient demographics
| Cycle 1 | Cycle 2 | |
| Total number | 102 | 100 |
| Sex | ||
| Male | 62 | 57 |
| Female | 40 | 43 |
| Age group, years | ||
| <40 | 7 | 5 |
| 40–49 | 9 | 11 |
| 50–59 | 24 | 24 |
| 60–69 | 28 | 26 |
| 70–79 | 22 | 19 |
| 80–89 | 11 | 12 |
| 90–99 | 1 | 3 |
| Admission source | ||
| AAU | 29 | 28 |
| ED | 73 | 72 |
| Receiving location | ||
| CCU | 17 | 5 |
| Ward | 85 | 95 |
| Pre-admission diabetic status | ||
| T1DM | 1 | 1 |
| T2DM | 19 | 24 |
| Treated as MI? | ||
| Type 1 MI | 42 | 20 |
| Key: AAU = acute assessment unit; CCU = coronary care unit; ED = emergency department; MI = myocardial infarction; T1DM = type 1 diabetes mellitus; T2DM = type 2 diabetes mellitus | ||
Results
Cycle 1: January–March 2023
Data were collected for 102 patients over a 12-week period. Age ranged from 18 to 92 years with a mean age of 62 ± 15.4 years. Table 2 outlines the patient demographics of the cycle 1 cohort. Prior to admission, 20% (n=19) had type 2 and 2% (n=1) had type 1 DM. Overall, 41% of patients were treated as a T1MI. The mean total cholesterol for cycle 1 was 4.8 mmol/L, mean LDL-C 2.9 mmol/L and mean HbA1c 44 mmol/mol.
Cycle 2: May–July 2023
Data collected for 100 patients were audited over an eight-week period. Age ranged from 34 to 94 years with a mean age of 63 ± 14.3 years. Table 2 outlines the patient demographics of the cycle 2 cohort. Prior to admission, 24% (n=24) of patients had type 2 and 1% (n=1) had type 1 DM. Overall, 40% (n=40) were treated as a T1MI. The mean total cholesterol for cycle 2 was 4.4 mmol/l, mean LDL-C 2.3 mmol/L and mean HbA1c 48 mmol/mol.
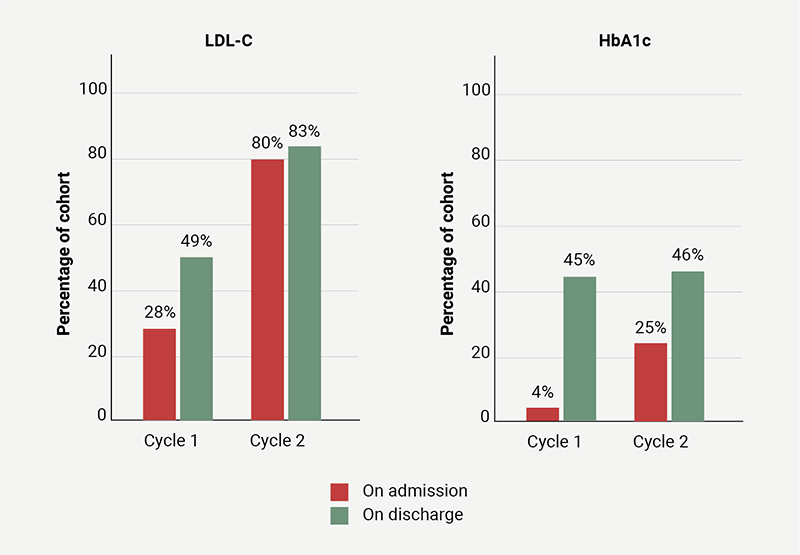
LDL-C and HbA1c testing on admission and discharge for both cycles are outlined in figure 1.
Following intervention there was an overall improvement in LDL-C testing from 49% to 83% by time of discharge, driven mainly by improvement in testing at admission from 28% to 80%. There was a significant improvement in patient testing with T1MI; 19% of those with T1MI had no lipid testing in cycle 1 compared with 0% in cycle 2. Only 17% of patients in cycle 2 had no LDL-C checked on their admission, which is very positive, however, still short of our 100% target as a specialist centre.
HbA1c testing improved on admission from 4% to 25% of patients tested. However, testing adherence by the time of discharge was comparable (45% in cycle 1 and 46% in cycle 2). The number of patients with a recent available HbA1c was also audited to reduce confounding factors. Allowing for recent testing of HbA1c, 66% of the cycle 1 cohort (n=68) and only 53% of the cycle 2 cohort (n=53) had HbA1c checked during their admission or in the three months prior to admission.
Throughout the course of the project, a number of patients were newly diagnosed with T2DM (n=6) as a direct result of HbA1c testing.
Discussion
LDL-C testing improvement was mainly attributable to improved testing at first assessment. This suggests that improved CV risk profiling can be achieved by inclusion of LDL-C (and HbA1c) testing in the admission ‘chest pain set’. Unfortunately, without appropriate lipid profile testing we will continue to underutilise available lipid-lowering therapies, resulting in unnecessary harm.
While HbA1c testing at point of admission improved, overall numbers tested remained at around 45%, suggesting further education and intervention is required to achieve the target of 100%. Our belief is that for patients presenting with high-risk chest pain, requiring admission to a cardiology ward, testing could be done prior to transfer. We recognise the importance of ensuring testing takes place before patients are discharged from our care and the need for shared responsibility to ensure optimal patient care. The number of patients newly diagnosed with T2DM emphasises that these tests contribute to both primary and secondary prevention of modifiable cardiac risk factors.
Unfortunately, due to subsequent concerns regarding budget and clinical governance from the ED, our intervention was interrupted and not continued past its pilot period, likely contributing to falling short of targets, in particular with HbA1c testing. Plans are now in place to introduce LDL-C testing, with further departmental teaching within the cardiology department to encourage wider HbA1c testing. Thereby, further cycles will allow this change to be audited, aiming for 100% overall testing of a full lipid profile and HbA1c in our cardiac patients, which should improve patient outcomes in the longer term.
Key messages
- Updating admission order sets to include low-density lipoprotein-cholesterol (LDL-C) testing improves lipid testing and, thus, primary and secondary prevention measures
- Lipid testing is improving overall in our cardiology centre
- More work is needed in improving glycated haemoglobin (HbA1c) testing in the high-risk chest pain population, this study has demonstrated clear benefit in establishing diabetic status in our patients
Conflicts of interest
None declared.
Funding
None.
Study approval
The Deputy Medical Director of NHS GGC has confirmed that ethical approval is not required as this is an audit study.
References
1. Ference BA, Ginsberg HN, Graham H et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur Heart J 2017;38:2459–72. https://doi.org/10.1093/eurheartj/ehx144
2. Visseren FLJ, Mach F, Smulders YM et al. 2021 ESC guidelines on cardiovascular disease prevention in clinical practice: developed by the Task Force for cardiovascular disease prevention in clinical practice with representatives of the European Society of Cardiology and 12 medical societies. Eur Heart J 2021;42:3227–337. https://doi.org/10.1093/eurheartj/ehab484
3. National Institute for Health and Care Excellence (NICE). Lipid modification – CVD prevention. Clinical Knowledge Summary. London: NICE, 2020. Available from: https://cks.nice.org.uk/topics/lipid-modification-cvd-prevention/
4. Wang N, Woodward M, Huffman MD, Rodgers A. Compounding benefits of cholesterol-lowering therapy for the reduction of major cardiovascular events: systematic review and meta-analysis. Circ Cardiovasc Qual Outcomes 2022;15:e008552. https://doi.org/10.1161/CIRCOUTCOMES.121.008552
5. Rosenson RS. Myocardial injury: the acute phase response and lipoprotein metabolism. J Am Coll Cardiol 1993;22:933–40. https://doi.org/10.1016/0735-1097(93)90213-K
6. The Emerging Risk Factors Collaboration. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: a collaborative meta-analysis of 102 prospective studies. Lancet 2010;375:2215–22. https://doi.org/10.1016/S0140-6736(10)60484-9
7. Sethi SS, Akl EG, Farkouh ME. Diabetes mellitus and acute coronary syndrome: lessons from randomized clinical trials. Curr Diab Rep 2012;12:294–304. https://doi.org/10.1016/S0140-6736(10)60484-9
8. Jacoby RM, Nesto RW. Acute myocardial infarction in the diabetic patient: pathophysiology, clinical course and prognosis. J Am Coll Cardiol 1992;20:736–44. https://doi.org/10.1016/0735-1097(92)90033-J
9. Avanzini F, Mafrici A, Riva E et al. A multicenter observational study on the management of hyperglycemia in patients with acute coronary syndrome. Nutr Metab Cardiovasc Dis 2015;25:916–23. https://doi.org/10.1016/j.numecd.2015.07.007
10. Kmet M, Rajer B, Pernat A. Hemoglobin A1c is a better predictor of prognosis following the non-ST elevation acute coronary syndrome than fasting and admission glucose. Wien Klin Wochenschr 2014;126:156–62. https://doi.org/10.1007/s00508-013-0468-2
11. Nichols GA, Joshua-Gotlib S, Parasuraman S. Glycemic control and risk of cardiovascular disease hospitalization and all-cause mortality. J Am Coll Cardiol 2013;62:121–7. https://doi.org/10.1016/j.jacc.2013.04.031
12. Pan W, Lu H, Lian B, Liao P, Guo L, Zhang M. Prognostic value of HbA1c for in-hospital and short-term mortality in patients with acute coronary syndrome: a systematic review and meta-analysis. Cardiovasc Diabetol 2019;18:169. https://doi.org/10.1186/s12933-019-0970-6
13. National Institute for Health and Care Excellence. Acute coronary syndromes. NG185. London: NICE, 2020. Available from: https://www.nice.org.uk/guidance/ng185/
14. Marx N, Federici M, Schütt K et al. 2023 ESC guidelines for the management of cardiovascular disease in patients with diabetes: developed by the task force on the management of cardiovascular disease in patients with diabetes of the European Society of Cardiology. Eur Heart J 2023;44:4043–140. https://doi.org/10.1093/eurheartj/ehad774
15. Aubiniere-Robb L, Dickerson J, Brady AJB. Lipid testing and treatment after acute myocardial infarction: no flags for the flagship. Br J Cardiol 2019;26:141–4. https://doi.org/10.5837/bjc.2019.041
16. Hodkinson A, Tsimpida D, Kontopantelis E, Rutter MK, Mamas MA, Panagioti M. Comparative effectiveness of statins on non-high density lipoprotein cholesterol in people with diabetes and at risk of cardiovascular disease: systematic review and network meta-analysis. BMJ 2022;376:e067731. https://doi.org/10.1136/bmj-2021-067731
17. Bohula EA, Morrow DA, Cannon CP et al. Atherothrombotic risk stratification and ezetimibe use in IMPROVE-IT. J Am Coll Cardiol 2017;69:911–21. https://doi.org/10.1016/j.jacc.2016.11.070
18. Schwartz GG, Steg PG, Szarek M et al. Alirocumab and cardiovascular outcomes after acute coronary syndrome. N Engl J Med 2018;379:2097–107. https://doi.org/10.1056/NEJMoa1801174
19. Sabatine MS, Giugliano RP, Keech AC et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med 2017;376:1713–22. https://doi.org/10.1056/NEJMoa1615664
20. Saeed A, Ballantyne CM. Bempedoic acid (ETC-1002): a current review. Cardiol Clin 2018;36:257–64. https://doi.org/10.1016/j.ccl.2017.12.007
21. Nissen SE, Lincoff AM, Brennan D et al. Bempedoic acid and cardiovascular outcomes in statin-intolerant patients. N Engl J Med 2023;388:1353–64. https://doi.org/10.1056/NEJMoa2215024
22. Bhatt DL, Steg PG, Miller M et al. Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia. N Engl J Med 2019;380:11–22. https://doi.org/10.1056/NEJMoa1812792
