The management and prevention of cardiovascular diseases (CVD) is based on adequate adherence to medications and lifestyle changes. The reported rates of adherence with cardiovascular medications range from 30% to 70%, with patients often not taking all or part of their prescribed medications. The rates of non-adherence are even higher for individual cardiovascular risk factors. Assessment of medication adherence is an important part of the management of CVD. Many interrelated socio-economic and healthcare-related factors play a role in an individual patient’s adherence to medications. Understanding how these different factors affect each individual patient can lead to strategies that improve levels of adherence. This would help improve our control of CVDs, both at an individual patient level, and also at the level of national and international health.
Introduction

Cardiovascular disease (CVD) represents a major cause of morbidity and mortality worldwide. It is estimated that 17.9 million deaths (representing 32% of all deaths) in 2019 were attributed to CVD.1 With a high prevalent global burden of the disease, there is a major impetus on prevention. A major part of the management and prevention of CVD lies in adherence to medications and lifestyle changes, with the intention of lowering future cardiovascular events, and for symptom control.2 Medications are prescribed, either as primary prevention for those at high risk for future cardiovascular events, or secondary prevention of future events for those who have already sustained a cardiovascular event. Current evidence-based practice has led to patients with CVD, and those at high risk, being initiated on an increasing number of medications.3 As with most chronic illnesses, non-adherence to medication and lifestyle modifications, remains a major issue when these are part of a long-term preventive strategy, rather than symptom control.3
The reported rates of adherence with cardiovascular medications range from 30% to 70%, with patients often not taking all or part of their prescribed medications.4,5 In a meta-analysis of around 20 observational studies involving more than 300,000 patients, it was estimated that the prevalence of poor adherence was as high as 43%.5
For individual risk factors that rate can be even higher. It has been demonstrated that at the end of six months, one-third of patients discontinue their antihypertensive medications, and only around half of all patients persist with their initial therapy at one year.6 Naderi et al. have demonstrated that, in patients with CVD, the rates of adherence for primary prevention are generally lower than those for secondary prevention, with those who have suffered a myocardial infarction (MI) or a stroke more likely to take their medication regularly than those who have not suffered an event.5 However, even for those on secondary prevention, adherence is suboptimal, as demonstrated in a study on 4,591 post-MI patients, where around 18% of patients did not collect their prescriptions even once in the four months following the MI.7 In a separate cohort of 22,379 post-acute coronary syndrome (ACS) patients, 60% discontinued their statin medication within two years of hospitalisation.8
Poor adherence is a major public health issue, such that the World Health Organisation (WHO), in their report on adherence to long-term therapies, state that interventions to improve medication adherence might have a far greater impact on the health of the population than any improvement in a specific medical treatment itself.9,10 Adherence is an independent, active, voluntary and collaborative involvement of the patient, resulting in their taking a range of actions to produce a desired therapeutic result that has been agreed upon by the patient and the healthcare provider.10 The term ‘compliance’ is generally not favoured anymore, as this implies that the patient passively accepts the recommendations of the prescriber, with little or no engagement by the patient themselves.11
Factors affecting adherence
Table 1. Factors affecting medication adherence
| Socio-economic factors |
|
| Patient-related factors |
|
| Therapy-related factors |
|
| Comorbidities |
|
| Healthcare-related factors |
|
The degree of adherence to medication by any individual patient can change over time, based on various personal and other factors. The WHO has identified five broad categories of factors that affect adherence (table 1):10
- Socio-economic factors
- Patient-related
- Therapy-related
- Comorbid conditions
- Healthcare system-related.
These factors are interdependent and ultimately play a role in the individual patient’s willingness or ability to be adherent to medications. Socio-economic factors, such as age, sex, ethnicity, social, economic, educational and occupational status, can affect adherence in many ways.12 It affects their understanding of the disease, access to healthcare, their health beliefs, forgetfulness and fears of dependence. The therapy-related factors and comorbid conditions relate to the total pill burden, side effects, cost of medications, and the ease of access to medications and refills.13 This is also related to the healthcare system factors, which determine the cost of therapy, the availability of fixed-dose combinations, access to healthcare in case of side effects, and the ease of filling prescriptions, etc.13
Patients’ beliefs and fears regarding the diagnosis, and the impact of this diagnosis on their lifestyle, also play a role in adherence.14 The diagnosis of ischaemic heart disease (IHD) may have an impact on their health insurance and job prospects, leading to some patients denying that anything is wrong with them, and, therefore, not taking their medications. In some cultures, there is a suspicion towards modern medicine, with a tendency to try traditional therapies first.15 Side effects, such as postural hypotension in the elderly, erectile dysfunction and frequent micturition, may also limit acceptance of, and adherence to, medication by some patients.13
Assessment of adherence
While the importance of treatment adherence is well accepted, it is, however, challenging to assess it in clinical practice. This is often due to time constraints, and due to the dynamic nature of adherence, with patients having periods of varying levels of adherence/non-adherence depending on their personal situation. In addition, there is no clear gold-standard method of assessing adherence. There is also no set criterion to determine what level of adherence is considered as ‘good adherence’ or ‘bad adherence’, beyond which medications don’t have their desired effect. For example, is a person who takes his statin five times a week (rather than daily) more adherent than a person who takes it two times a week. It could be argued that the desired effect, i.e. either blood pressure or serum cholesterol or low-density lipoprotein (LDL) level, is more important than assessing how often they take their tablets. Some authors have even suggested that higher-dose statins be prescribed to accommodate non-adherence, rather than ensure good adherence on a low-dose statin, in order to achieve target cholesterol and LDL levels.16
Direct patient questioning based on self-recall and self-reporting is the most common method of assessing medication adherence in daily clinical practice. This is, however, very unreliable, and multiple studies have shown that patients and physicians tend to over report medication adherence, with some authors stating that this method is no better than the toss of a coin.17
The use of standard structured questionnaires is another method often utilised in clinical trials, and has been recommended to be used in daily clinical practice. However, lack of time and the nature of these questions often limit the practicality of their use at each clinic visit. There are many questionnaires available and some, such as the Hill-Bone compliance scale, are specifically tailored for use with hypertensive patients.18 Table 2 summarises some of these widely available questionnaires, along with their advantages and disadvantages. The updated Morisky Medication Adherence Scale (MMAS-8)19 and the Self-Efficiency for Appropriate Medication use (SEAMS) questionnaire20 have high internal consistency and are frequently used. These questionnaires are good as screening tools as they provide a sense of the level of adherence, but they do not delve into the causes behind non-adherence.21 The Brief Medication Questionnaire (BMQ), in addition to assessing adherence also tries to assess the reasons behind poor adherence.22
Table 2. Commonly used questionnaires to assess adherence to treatment in patients with chronic illnesses
| Questionnaire | Features/advantages | Disadvantages | Validated conditions for use |
| MMAS-837 | 8 questions High internal consistency (Cronbach’s alpha 0.83) High sensitivity and specificity (93% and 53%, respectively) Available in many languages (French, Portuguese, Urdu, Turkish, Chinese, Malay) Useful as a screening tool Easy to use; quick (approx. 1 minute) |
Does not fully explore the factors contributing to non-adherence | Hypertension Hyperlipidaemia Diabetes mellitus Parkinson’s disease Heart failure Ischaemic heart disease |
| HBCS36 | 14 questions High internal consistency (Cronbach’s alpha 0.79) Sensitivity and specificity of 67.4% and 67.8%, respectively Available in many languages (e.g. Arabic, Chinese, German, Korean, Malay, Persian, Polish, Portuguese, and Turkish) Identifies barriers to adherence Includes questions related to salt intake |
Developed specifically for hypertension and African ethnicity Validated in other conditions, although questions are fairly hypertension specific Not validated in other ethnicities Time-consuming (approx. 5 minutes) |
Hypertension Diabetes mellitus Stroke HIV |
| SEAMS38 | 13 questions High internal consistency (Cronbach’s alpha 0.89) Based on the socio-cognitive theory Can be used in patients with limited literacy Identifies barriers to adherence |
Time-consuming (approx. 5 minutes) Not practical for everyday use |
Ischaemic heart disease Hypertension Diabetes mellitus |
| BMQ40 | 2–5 item scales Short and easy to use (approx. 1 minute) Available in many languages (e.g. Swedish, Malay, Dutch, Spanish, Maltese) Sensitivity and specificity of 77% and 58%, respectively Assesses patients’ beliefs and attitudes towards their condition specifically and medications in general |
Does not identify the barriers to non-adherence Low internal consistency compared with the other questionnaires (Cronbach’s alpha 0.66) |
Diabetes mellitus Hypertension |
| ACDS60 | Developed specifically for chronic diseases and validated for CHD 7 questions (5 about practice and 2 about situations affecting adherence) Takes into account both assessment of adherence and questions regarding belief and attitudes |
Not validated in other languages apart from Polish and English Low internal consistency (Cronbach’s alpha 0.75) |
CHD |
| Key: ACDS = Adherence in Chronic Disease Scale; BMQ = Beliefs about Medicine Questionnaire; CHD = coronary heart disease; HBCS = Hill-Bone Compliance Scale; HIV = human immunodeficiency virus; MMAS = Morisky Medication Adherence Scale; SEAMS = Self-Efficacy About Medication Use | |||
Other indirect methods include pill count, where patients bring their medications to consultations and the physician or healthcare professional (HCP) counts the number of tablets remaining.21 This is the method often used in clinical trials, but not practical for routine clinical practice. Measuring the number of refill prescriptions issued to patients works in a similar manner, where patients who are strictly adherent to medications will often get a refill prescription ahead of when the previous one expires.23 The use of electronic health records and pharmacy databases can help to highlight patients who have missed appointments or have not collected their refill prescriptions on time.24
The directly observed therapy (DOT) method was popularised in many countries for the treatment of diseases of public health interest, such as tuberculosis and leprosy.25 Here, health workers would administer the medications directly under their supervision and maintain strict pill counts. A video-link DOT method has also been piloted in some countries, with variable success.26 Access to a video-recording device and good internet services are, however, limitations of this variation. The DOT and video-DOT are, however, feasible for conditions such as tuberculosis, where the treatment is for a relatively short, fixed-term duration, and, therefore, may not be practical in chronic illnesses like CVD, where lifelong therapy is indicated.
Measuring the level of drugs, or their metabolites, in the plasma or urine are another method that is used in drug trials.21,23 However, these are cumbersome and expensive, and, therefore, not always practical for use in routine practice. Urinalysis of most of the commonly used antihypertensives and antianginals is available, and although their complete absence in a spot urine sample can suggest total non-adherence, the mere presence of the metabolites does not always suggest complete adherence.27
There are new emerging technologies, such as electronic monitoring systems, that can help monitor adherence. One such device is the Medication Event Monitoring System (MEMS), where microcircuits embedded in the medication packaging keep a record of the number of doses that are taken, along with the date and time.28 This would accurately record when the tablet is removed from the packaging, but is open to manipulation by the patient (i.e. removed from the package, but not consumed). In a study on predominantly African-American women, 93% reported that the MEMS was easy to open, 85% did not find it stressful, and 75% liked the MEMS and used it every day. However, a smaller proportion (one-third) of patients preferred using a pillbox, and 25% did not like travelling with the MEMS.29
Ingestible sensors have also been trialled to monitor adherence.30 The Proteus device™ (Proteus Digital Health, Redwood City, USA) is an innovative method that incorporates an ingestible sensor along with the tablet itself.31 The ingested sensor is activated in the stomach and the signal picked up by a skin patch, which is then transmitted to a Bluetooth-enabled device. The results of the trials are promising, and this might be the future of adherence monitoring. At present, however, these emerging technologies are expensive and not readily available.
Strategies to improve adherence
During the brief clinical encounter in the busy outpatient setting, it is difficult to get a true sense of the level of adherence to medication, and the factors that might prevent the patient from being fully adherent to prescribed medications. However, the physician should be vigilant to picking up clues pointing to non-adherence, such as missed appointments, late prescription refill, higher than usual blood pressure, etc.
Adherence is a very individual characteristic and often members of the same household will exhibit different levels of adherence. It may also vary in the same patient at different times. Therefore, ascertaining the reasons for non-adherence in each patient, and assessing their beliefs and concerns regarding their diagnosis and management, play an important part in improving adherence.32 HCPs can help patients overcome many of the barriers to adherence by working in collaboration with their patients and family members/caregivers, and other providers, to identify, remove, or minimise the barriers. Discussions with the patient and their caregiver should be open and with a non-confrontational ‘no-blame’ approach to come to a common agreed plan.
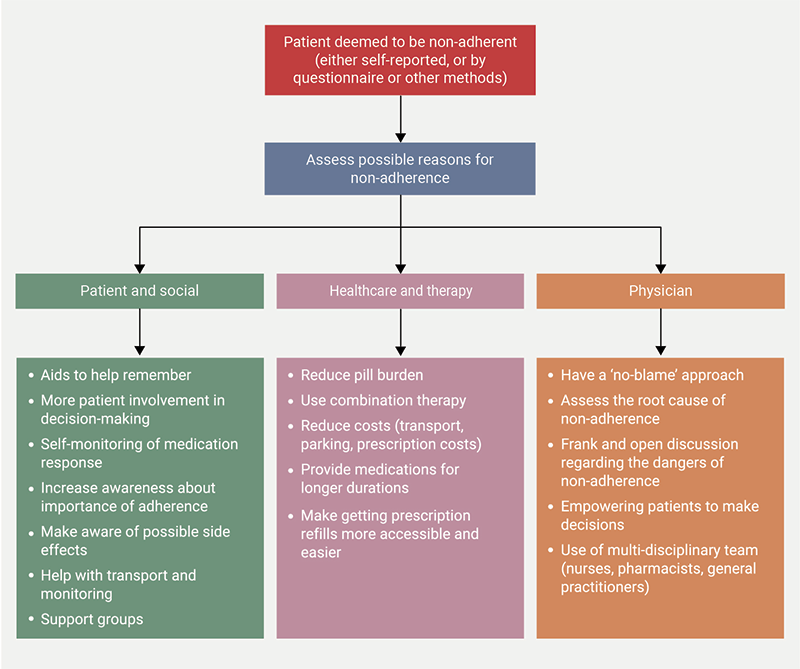
While there is no single gold-standard strategy for improving adherence, it is generally recognised that using multi-pronged individualised interventions is the best approach.32 The strategies used to improve adherence will depend on the five components of factors that affect adherence that were mentioned earlier (figure 1). The most important aspect of improving adherence is understanding the patient’s perspective. Forgetfulness plays a major part in non-adherence for most patients. Busy lifestyles might hinder adherence, especially when patients are asymptomatic, and it is important to educate the patient on the need for, and importance of, adherence.32 Potential side effects should be explicitly explained, so patients will know what to expect and how some side effects could be ameliorated. Patients could be provided with aids, such as daily text messages, email alerts or entries in the diary, dosette-boxes, etc., to remind them to take their medications.33 Associating medication intake with a particular daily activity, for example, to take it with breakfast, can help the patient remember.34 In patients with cognitive impairment, the responsibility for administering medication could be transferred to their caregiver, who ought to be educated on the importance of medication adherence and the regimen required.35
Involvement of a multi-disciplinary team that includes pharmacists, specialist nurses, community healthcare workers and general practitioners/family doctors, can have a positive impact to increase medication adherence.36 During each visit or contact with the patient, adherence to medication should be discussed. The team-based care approach allows patients to feel they have more than one HCP they can turn to in case of any problems with their medications. In addition, pharmacists and nurses have been shown to be more effective in providing high-quality patient education than hospital-based physicians, who are often more time-constrained.
The involvement of the patient and family/caregivers in the decision-making, in terms of choice of drug (and their potential side effects, such as increased diuresis with diuretics, etc.), timing of medications, etc., helps to improve adherence.36 Increased involvement of patients in self-monitoring, such as home blood-pressure and blood-sugar monitoring, has been shown to be effective in improving adherence. Home-monitoring provides the patient with immediate feedback regarding blood pressure and blood sugar, and also serves as a reminder to be adherent to medications. Empowering the patient to take more responsibility for their health and management by self-monitoring can also improve medication adherence.37
The use of fixed-dose combination pills that lower the number of tablets that need to be consumed, can help in patients who have a high daily-pill burden.38 Studies have shown that non-adherence is around 10% with one pill daily and 20% with two pills daily, with very high rates (>40%) of partial or complete non-adherence in patients receiving five or more pills daily.39 In a recent large trial, 2,499 patients were randomised to either the polypill or standard care, where they were given the individual medications. Medication adherence was shown to be higher in the polypill group, and was associated with a significant reduction in the primary composite outcome of cardiovascular death, nonfatal type 1 MI, nonfatal ischaemic stroke, or urgent revascularisation (9.5% for polypill vs. 12.7% for standard care, p=0.02) and composite secondary end point of cardiovascular death, nonfatal type 1 MI, or nonfatal ischaemic stroke (8.2% for polypill vs. 11.7% for standard care, p=0.005) at 36 months of follow-up in the polypill group.40
Similar results were also obtained from the NEPTUNO study, where a larger number of patients (n=6,466) were randomised to either the polypill or individual components. Those receiving the polypill had significantly lower adverse cardiac events at two years, with significantly better medication adherence rates.41 The use of the polypill strategy has also been demonstrated to be cost-effective in a post-hoc analysis of studies and data obtained from registries.42 The use of the polypill might be especially useful in conditions such as heart failure, to ensure that the patient is getting the four pillars of treatment, as recommended by the guidelines.43 However, the use of a fixed-dose polypill is not widely accepted by all physicians, mainly due to the restrictions in dose adjustments.44
The use of cheaper generic medications may also be useful if cost is a contributing factor to non-adherence, although some studies dispute the overall effectiveness of generics in improving adherence.45,46 It has been demonstrated that prejudices remain against the use of generics by patients and physicians, both of whom have a negative opinion regarding their efficacy, and consider them inferior to brand-named drugs.47 The change in brand, resulting in change in shape or colour of the pills, has also been demonstrated previously to decrease adherence, with patients either reporting more side effects or less efficacy, and preferring to go back to the original pill.48 It is, therefore, important for pharmacists or physicians to inform the patient when a new brand is being substituted.
Synchronising medication refills, along with providing longer supplies, can help those with busy schedules.49 Other approaches for improving adherence, which have been implemented with some success in other chronic conditions, include cognitive behavioural therapy and motivational interviewing.50,51
Modern technology can also play a role in improving adherence to medication.52 Technologies, such as the GlowCap™53 and MEMS™28 systems, have demonstrated improved adherence. The use of electronic applications on smart phones or devices to remind patients to take their medications has been demonstrated to be effective in many clinical settings.54 The use of electronic medication packaging devices that monitor adherence can also serve as a reminder to improve adherence.55 The awareness that their adherence is being monitored might encourage patients to be more adherent. Being part of a social network and self-help groups may also be beneficial in improving adherence.56
Despite the availability of extensive literature, a recent Cochrane review suggested that no type of intervention was found to improve adherence among elderly patients on multiple medications when it was measured as a continuous variable, with educational only and mixed interventions having little or no impact.57 A further review by Fuller et al., specifically investigating medication adherence in cardiovascular disease, found that only three interventions (messaging service, fixed-dose combination pills and community healthcare worker-based interventions) showed benefit.58
Xu et al. have recently suggested a step-wise tailored approach to improving medication adherence in CVD.59 The first step is to identify non-adherence, followed by detecting the barriers to medication adherence, which could be using direct patient questioning or using questionnaires. Tailored approaches, involving multi-disciplinary teams and a multi-modal approach, can then be drawn up based on the perceived threats and barriers for each individual.
Conclusion
Adherence to medications is an integral part of the management of any illness. Better communication between the HCP and the patient and/or their caregiver is key to understanding the barriers to medication adherence and to overcome these obstacles. The treating physician should be sensitive to the individual needs of the patient, so that therapy can be tailored according to their personal circumstances. Improving adherence requires a multi-pronged approach with multi-disciplinary team involvement and the complete engagement of the patient or their caregiver. High levels of adherence are possible with investment in time and effort, resulting in significant health benefits, not just for the patient, but for the population as a whole.
Key messages
- Adherence to medications is an integral part of the management of any illness
- There are many methods to assess adherence, however, with the advent of newer technologies, we may be able to better understand and assess adherence
- The causes of non-adherence are often unique to a particular patient
- Improving adherence requires a multi-pronged approach with multi-disciplinary team involvement and the complete engagement of the patient or their caregiver
- High levels of adherence are possible with investment in time and effort, resulting in significant health benefits, not just for the patient, but for the population as a whole
Conflicts of interest
None declared.
Funding
None.
References
1. World Health Organisation. Cardiovascular diseases (CVDs). Geneva: WHO, 2025. Available from: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds)
2. Roth GA, Mensah GA, Fuster V. The global burden of cardiovascular diseases and risks: a compass for global action. J Am Coll Cardiol 2020;76:2980–1. https://doi.org/10.1016/j.jacc.2020.11.021
3. Kotseva K, Jennings C, Bassett P et al. Challenge of cardiovascular prevention in primary care: achievement of lifestyle, blood pressure, lipids and diabetes targets for primary prevention in England – results from ASPIRE-3-PREVENT cross-sectional survey. Open Heart 2024;11:e002704. https://doi.org/10.1136/openhrt-2024-002704
4. Baroletti S, Dell’Orfano H. Medication adherence in cardiovascular disease. Circulation 2010;121:1455–8. https://doi.org/10.1161/CIRCULATIONAHA.109.904003
5. Naderi SH, Bestwick JP, Wald DS. Adherence to drugs that prevent cardiovascular disease: meta-analysis on 376,162 patients. Am J Med 2012;125:882.e1–887.e1. https://doi.org/10.1016/j.amjmed.2011.12.013
6. Schulz M, Krueger K, Schuessel K et al. Medication adherence and persistence according to different antihypertensive drug classes: a retrospective cohort study of 255,500 patients. Int J Cardiol 2016;220:668–76. https://doi.org/10.1016/j.ijcard.2016.06.263
7. Jackevicius CA, Li P, Tu JV. Prevalence, predictors, and outcomes of primary nonadherence after acute myocardial infarction. Circulation 2008;117:1028–36. https://doi.org/10.1161/CIRCULATIONAHA.107.706820
8. Jackevicius CA, Mamdani M, Tu JV. Adherence with statin therapy in elderly patients with and without acute coronary syndromes. JAMA 2002;288:462–7. https://doi.org/10.1001/jama.288.4.462
9. Brown MT, Bussell JK. Medication adherence: WHO cares? Mayo Clin Proc 2011;86:304–14. https://doi.org/10.4065/mcp.2010.0575
10. World Health Organisation. Adherence to long-term therapies: evidence for action. Geneva: WHO, 2003. Available from: https://iris.who.int/server/api/core/bitstreams/121c6b73-8651-442f-9560-e3b1d9c8a75c/content
11. Vrijens B, De Geest S, Hughes DA et al. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol 2012;73:691–705. https://doi.org/10.1111/j.1365-2125.2012.04167.x
12. Magrin ME, D’Addario M, Greco A et al. Social support and adherence to treatment in hypertensive patients: a meta-analysis. Ann Behav Med 2015;49:307–18. https://doi.org/10.1007/s12160-014-9663-2
13. Kvarnström K, Westerholm A, Airaksinen M, Liira H. Factors contributing to medication adherence in patients with a chronic condition: a scoping review of qualitative research. Pharmaceutics 2021;13:1100. https://doi.org/10.3390/pharmaceutics13071100
14. Garavalia L, Garavalia B, Spertus JA, Decker C. Exploring patients’ reasons for discontinuance of heart medications. J Cardiovasc Nurs 2009;24:371–9. https://doi.org/10.1097/JCN.0b013e3181ae7b2a
15. Alodhaib G, Alhusaynan I, Mirza A, Almogbel Y. Qualitative exploration of barriers to medication adherence among patients with uncontrolled diabetes in Saudi Arabia. Pharmacy (Basel) 2021;9:16. https://doi.org/10.3390/pharmacy9010016
16. Vodonos A, Ostapenko I, Toledano R et al. Statin adherence and LDL cholesterol levels. Should we assess adherence prior to statin upgrade? Eur J Intern Med 2015;26:268–72. https://doi.org/10.1016/j.ejim.2015.02.014
17. Zeller A, Ramseier E, Teagtmeyer A, Battegay E. Patients’ self-reported adherence to cardiovascular medication using electronic monitors as comparators. Hypertens Res 2008;31:2037–43. https://doi.org/10.1291/hypres.31.2037
18. Kim MT, Hill MN, Bone LR, Levine DM. Development and testing of the Hill-Bone compliance to high blood pressure therapy scale. Prog Cardiovasc Nurs 2000;15:90–6. https://doi.org/10.1111/j.1751-7117.2000.tb00211.x
19. Morisky DE, Ang A, Krousel-Wood M, Ward HJ. Predictive validity of a medication adherence measure in an outpatient setting. J Clin Hypertens (Greenwich) 2008;10:348–54. https://doi.org/10.1111/j.1751-7176.2008.07572.x
20. Risser J, Jacobson TA, Kripalani S. Development and psychometric evaluation of the self-efficacy for appropriate medication use scale (SEAMS) in low-literacy patients with chronic disease. J Nurs Meas 2007;15:203–19. https://doi.org/10.1891/106137407783095757
21. Anghel LA, Farcas AM, Oprean RN. An overview of the common methods used to measure treatment adherence. Med Pharm Rep 2019;92:117–22. https://doi.org/10.15386/mpr-1201
22. Svarstad BL, Chewning BA, Sleath BL, Claesson C. The brief medication questionnaire: a tool for screening patient adherence and barriers to adherence. Patient Educ Couns 1999;37:113–24. https://doi.org/10.1016/S0738-3991(98)00107-4
23. Lam WY, Fresco P. Medication adherence measures: an overview. Biomed Res Int 2015;2015:217047. https://doi.org/10.1155/2015/217047
24. Sikka R, Xia F, Aubert RE. Estimating medication persistency using administrative claims data. Am J Manag Care 2005;11:449–57. Available from: https://www.ajmc.com/view/jul05-2085p449-457
25. Karumbi J, Garner P. Directly observed therapy for treating tuberculosis. Cochrane Database Syst Rev 2015;2015:CD003343. https://doi.org/10.1002/14651858.CD003343.pub4
26. Sekandi JN, Buregyeya E, Zalwango S et al. Video directly observed therapy for supporting and monitoring adherence to tuberculosis treatment in Uganda: a pilot cohort study. ERJ Open Res 2020;6:00175-2019. https://doi.org/10.1183/23120541.00175-2019
27. van der Hooft JJ, Padmanabhan S, Burgess KE, Barrett MP. Urinary antihypertensive drug metabolite screening using molecular networking coupled to high-resolution mass spectrometry fragmentation. Metabolomics 2016;12:125. https://doi.org/10.1007/s11306-016-1064-z
28. Checchi KD, Huybrechts KF, Avorn J, Kesselheim AS. Electronic medication packaging devices and medication adherence: a systematic review. JAMA 2014;312:1237–47. https://doi.org/10.1001/jama.2014.10059
29. Ogedegbe G, Chaplin W, Schoenthaler A et al. A practice-based trial of motivational interviewing and adherence in hypertensive African Americans. Am J Hypertens 2008;21:1137–43. https://doi.org/10.1038/ajh.2008.240
30. Hafezi H, Robertson TL, Moon GD, Au-Yeung KY, Zdeblick MJ, Savage GM. An ingestible sensor for measuring medication adherence. IEEE Trans Biomed Eng 2015;62:99–109. https://doi.org/10.1109/TBME.2014.2341272
31. Alipour A, Gabrielson S, Patel PB. Ingestible sensors and medication adherence: focus on use in serious mental illness. Pharmacy (Basel) 2020;8:103. https://doi.org/10.3390/pharmacy8020103
32. Chang TE, Ritchey MD, Ayala C, Durthaler JM, Loustalot F. Use of strategies to improve antihypertensive medication adherence within United States outpatient health care practices, DocStyles 2015–2016. J Clin Hypertens (Greenwich) 2018;20:225–32. https://doi.org/10.1111/jch.13188
33. Shah R, Watson J, Free C. A systematic review and meta-analysis in the effectiveness of mobile phone interventions used to improve adherence to antiretroviral therapy in HIV infection. BMC Public Health 2019;19:915. https://doi.org/10.1186/s12889-019-6899-6
34. Han HR, Kim K, Murphy J et al. Community health worker interventions to promote psychosocial outcomes among people living with HIV – a systematic review. PLoS One 2018;13:e0194928. https://doi.org/10.1371/journal.pone.0194928
35. Muñoz-Contreras MC, Segarra I, López-Román FJ, Galera RN, Cerdá B. Role of caregivers on medication adherence management in polymedicated patients with Alzheimer’s disease or other types of dementia. Front Public Health 2022;10:987936. https://doi.org/10.3389/fpubh.2022.987936
36. Saag KG, Bhatia S, Mugavero MJ, Singh JA. Taking an interdisciplinary approach to understanding and improving medication adherence. J Gen Intern Med 2018;33:136–8. https://doi.org/10.1007/s11606-017-4215-7
37. Thiruvengadam SK, Ashvetiya T, Stone NJ, Blumenthal RS, Martin SS. Shared decision-making and patient empowerment in preventive cardiology. Curr Cardiol Rep 2016;18:49. https://doi.org/10.1007/s11886-016-0729-6
38. Parati G, Kjeldsen S, Coca A, Cushman WC, Wang J. Adherence to single-pill versus free-equivalent combination therapy in hypertension: a systematic review and meta-analysis. Hypertension 2021;77:692–705. https://doi.org/10.1161/HYPERTENSIONAHA.120.15781
39. Benner JS, Chapman RH, Petrilla AA, Tang SS, Rosenberg N, Schwartz JS. Association between prescription burden and medication adherence in patients initiating antihypertensive and lipid-lowering therapy. Am J Health Syst Pharm 2009;66:1471–7. https://doi.org/10.2146/ajhp080238
40. Castellano JM, Cordero A, Fuster V. Polypill strategy in secondary cardiovascular prevention. Reply. N Engl J Med 2022;387:2197–8. https://doi.org/10.1056/NEJMc2213446
41. González-Juanatey JR, Cordero A, Castellano JM et al. The CNIC-Polypill reduces recurrent major cardiovascular events in real-life secondary prevention patients in Spain: the NEPTUNO study. Int J Cardiol 2022;361:116–23. https://doi.org/10.1016/j.ijcard.2022.05.015
42. Aguiar C, Araujo F, Rubio-Mercade G et al. Cost-effectiveness of the CNIC-Polypill strategy compared with separate monocomponents in secondary prevention of cardiovascular and cerebrovascular disease in Portugal: the MERCURY study. J Health Econ Outcomes Res 2022;9:134–46. https://doi.org/10.36469/jheor.2022.39768
43. Pandey A, Keshvani N, Wang TJ. Should polypills be used for heart failure with reduced ejection fraction? Circulation 2022;146:276–8. https://doi.org/10.1161/CIRCULATIONAHA.122.059661
44. Sharma N, Khatib R, Elamin N et al. Optimal dosing of angiotensin-converting enzyme inhibitors and β-blockers for acute coronary syndrome: up-titration remains a challenge. Eur J Hosp Pharm 2016;23:203–06. https://doi.org/10.1136/ejhpharm-2015-000783
45. Briesacher BA, Andrade SE, Fouayzi H, Chan KA. Medication adherence and use of generic drug therapies. Am J Manag Care 2009;15:450–6. Available from: https://pmc.ncbi.nlm.nih.gov/articles/pmid/19589012/
46. Goldszmidt RB, Buttendorf AR, Schuldt Filho G, Souza JM, Bianchini MA. The impact of generic labels on the consumption of and adherence to medication: a randomized controlled trial. Eur J Public Health 2019;29:12–17. https://doi.org/10.1093/eurpub/cky183
47. Colgan S, Faasse K, Martin LR, Stephens MH, Grey A, Petrie KJ. Perceptions of generic medication in the general population, doctors and pharmacists: a systematic review. BMJ Open 2015;5:e008915. https://doi.org/10.1136/bmjopen-2015-008915
48. Kesselheim AS, Misono AS, Shrank WH et al. Variations in pill appearance of antiepileptic drugs and the risk of nonadherence. JAMA Intern Med 2013;173:202–08. https://doi.org/10.1001/2013.jamainternmed.997
49. Rubin R. Synchronizing medication refills could improve adherence. JAMA 2019;322:716. https://doi.org/10.1001/jama.2019.12349
50. Palacio A, Garay D, Langer B, Taylor J, Wood BA, Tamariz L. Motivational interviewing improves medication adherence: a systematic review and meta-analysis. J Gen Intern Med 2016;31:929–40. https://doi.org/10.1007/s11606-016-3685-3
51. Qin K, Zeng J, Liu L, Cai Y. Effects of cognitive behavioral therapy on improving depressive symptoms and increasing adherence to antiretroviral medication in people with HIV. Front Psychiatry 2022;13:990994. https://doi.org/10.3389/fpsyt.2022.990994
52. Mason M, Cho Y, Rayo J, Gong Y, Harris M, Jiang Y. Technologies for medication adherence monitoring and technology assessment criteria: narrative review. JMIR Mhealth Uhealth 2022;10:e35157. https://doi.org/10.2196/35157
53. Inoue S, Kodjebacheva G, Scherrer T et al. Adherence to hydroxyurea medication by children with sickle cell disease (SCD) using an electronic device: a feasibility study. Int J Hematol 2016;104:200–07. https://doi.org/10.1007/s12185-016-2027-x
54. Pérez-Jover V, Sala-González M, Guilabert M, Mira JJ. Mobile apps for increasing treatment adherence: systematic review. J Med Internet Res 2019;21:e12505. https://doi.org/10.2196/12505
55. van Onzenoort HA, Verberk WJ, Kroon AA et al. Electronic monitoring of adherence, treatment of hypertension, and blood pressure control. Am J Hypertens 2012;25:54–9. https://doi.org/10.1038/ajh.2011.153
56. Shahin W, Kennedy GA, Stupans I. The association between social support and medication adherence in patients with hypertension: a systematic review. Pharm Pract (Granada) 2021;19:2300. https://doi.org/10.18549/PharmPract.2021.2.2300
57. Cross AJ, Elliott RA, Petrie K, Kuruvilla L, George J. Interventions for improving medication-taking ability and adherence in older adults prescribed multiple medications. Cochrane Database Syst Rev 2020;5:CD012419. https://doi.org/10.1002/14651858.CD012419.pub2
58. Fuller RH, Perel P, Navarro-Ruan T, Nieuwlaat R, Haynes RB, Huffman MD. Improving medication adherence in patients with cardiovascular disease: a systematic review. Heart 2018;104:1238–43. https://doi.org/10.1136/heartjnl-2017-312571
59. Xu HY, Yu YJ, Zhang QH, Hu HY, Li M. Tailored interventions to improve medication adherence for cardiovascular diseases. Front Pharmacol 2020;11:510339. https://doi.org/10.3389/fphar.2020.510339
60. Kosobucka A, Michalski P, Pietrzykowski L et al. Adherence to treatment assessed with the adherence in chronic diseases scale in patients after myocardial infarction. Patient Prefer Adherence 2018;12:333–40. https://doi.org/10.2147/PPA.S150435
