Often considered benign, Takotsubo syndrome (TTS) could be life threatening. We present a 54-year-old female patient with a history of heterozygous beta-thalassaemia and Graves’ disease who came to the emergency department complaining of dizziness, atypical chest pain and an episode of collapse. The patient developed cardiac arrest due to ventricular fibrillation. After 45 minutes of cardiopulmonary resuscitation, return of spontaneous circulation was achieved. A transthoracic echocardiography revealed hypokinetic mid and apical left ventricular (LV) segments. Her coronary angiography showed significant stenosis in the left anterior descending coronary artery, for which she underwent percutaneous coronary intervention. In the subacute phase, she had episodes of polymorphic ventricular tachycardia in the context of QT-interval prolongation. Cardiac magnetic resonance imaging demonstrated diffuse myocardial oedema in the mid and apical segments of the LV. Finally, after 60 days of hospitalisation, an implantable cardioverter-defibrillator was implanted for secondary prevention of sudden cardiac death. This case study demonstrates some of the serious complications of TTS and the medical decisions that may need to be made regarding its treatment course.
Introduction
Takotsubo syndrome (TTS) is a reversible cardiomyopathy thought to arise in response to sudden adrenergic discharge. The prognosis is generally thought to be favourable but the initial presentation can be accompanied by life-threatening arrythmias.
The clinical presentation of a patient with TTS can imitate acute coronary syndromes (ACS) in the absence of obstructive coronary artery disease (CAD) on coronary angiography (CAG). The presence of co-existing stable CAD has also been reported and currently is not regarded as an exclusion criterion for the diagnosis of TTS. Moreover, TTS is often associated with abnormalities in ventricular repolarisation. Life-threatening ventricular tachyarrhythmias most frequently occur during the acute phase of TTS. Cardiac arrest affects a significant number of patients and is associated with high mortality rates.
The current international diagnostic criteria for TTS are the InterTAK diagnostic criteria. A score of 30 points confers a probability of TTS to be <1%, whereas a score of >70 points denotes a probability of TTS of around 90%. The diagnostic modalities that can be used to confirm TTS are cardiac echocardiography, coronary computed tomography angiography (CCTA), invasive CAG, invasive ventriculogram, intracoronary imaging, cardiac magnetic resonance imaging (CMR) and, in certain cases, nuclear imaging (especially in the presence of non-specific wall motion abnormalities).
The management should be adjusted on a case-by-case basis in most patients and remains predominantly supportive. Management of ACS and heart failure (HF) are individualised according to the findings of each patient. In some patients with large apical ballooning, anticoagulation therapy is needed. The use of implantable cardioverter-defibrillators (ICDs) for ventricular arrythmia (VA) management has been generally discouraged in the setting of TTS due to the reversible nature of this phenomenon. However, ICD implantation seems to be a plausible strategy in the setting of TTS that is considered as the consequence rather than the cause of a life-threatening ventricular arrythmia episode.
In this case report, the patient experienced cardiac arrest due to ventricular fibrillation as the first symptom of TTS. Her CAG showed sequential stenotic lesions in the middle and distal parts of the LAD coronary artery; PCI was successful in relieving the stenosis. The diagnose of TTS was confirmed by CMR. Moreover, an ICD was implanted for secondary prevention of sudden cardiac death. This case is an interesting one because it highlights many aspects of TTS that still remain controversial.
Case
A 54-year-old female patient presented to the emergency department with progressive weakness and atypical chest pain. She mentioned experiencing some particularly stressful family events in the last weeks and a strenuous day. Her medical history included heterozygous beta-thalassaemia and Graves’ disease. She had no significant medical family history, no allergies and no smoking reported. Her vital signs and electrocardiogram (ECG) were normal.
During venepuncture she complained about dizziness and then became unresponsive. The cardiac monitor revealed ventricular fibrillation. Cardiopulmonary resuscitation (CPR) was initiated with a return of spontaneous circulation after 45 minutes of continuous chest compressions, guideline-directed drug and defibrillation therapies, endotracheal intubation and ventilation. Her initial blood tests showed a mild elevation of high-sensitivity cardiac troponin I (hs-cTnI) of 23.0 pg/ml (normal range for females: 0–15.6 pg/ml).
The patient was transferred to the intensive care unit. Her transthoracic echocardiogram showed a reduced ejection fraction (EF: 40–45%), hypokinetic apical left ventricular (LV) segments with no clear coronary distribution, and an akinetic apex with hyperkinetic basal segments (apical ballooning type); these features were consistent with those seen in TTS.
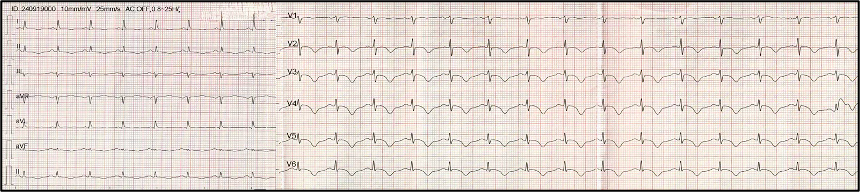
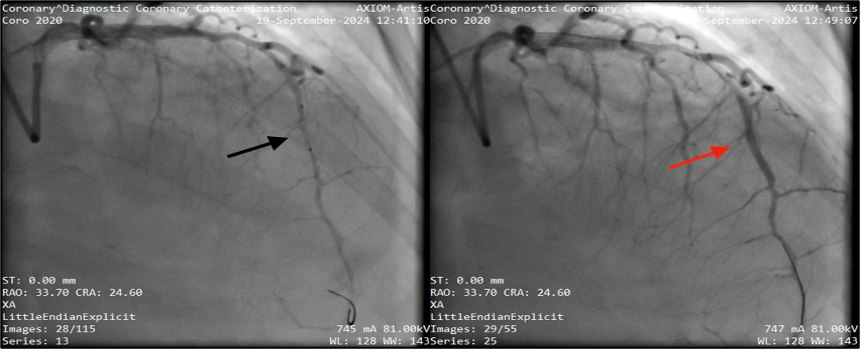
The next day she required neither hemodynamic support nor mechanical ventilation. An ECG was performed, which showed symmetrical negative T waves in all precordial and limb leads with QT prolongation (QTc: 539 ms) (figure 1). Plasma hs-cTnI levels rose up to 26,088 pg/ml and N-terminal of the prohormone of B-type natriuretic peptide (NT-proBNP) was 4,700 pg/ml (normal range: 0–350 pg/ml). She had an angiogram that showed sequential stenotic lesions (stenosis up to 80%) in the middle and distal parts of the LAD coronary artery. Coronary angioplasty was performed with placement of a drug-eluting stent (DES) (figure 2).
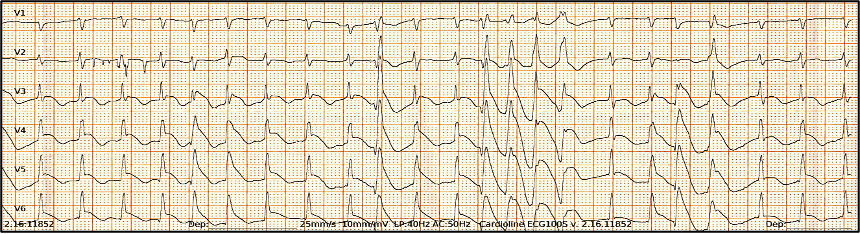
On day five, the patient complained of difficulty breathing. An ECG was performed which showed episodes of polymorphic ventricular tachycardias (figure 3). Magnesium 2 g was given intravenously. A new blood test revealed a mild hypokalaemia of 2.96 mmol/L (normal range: 3.4–5.1 mmol/L) and hypocalcaemia of 6.8 mg/dL (normal range: 8.4–10.2 mg/dL). The resting ECG in sinus rhythm depicted significant prolongation of the corrected QT interval (QTc: 640 ms). The electrolyte imbalances were corrected and the QTc interval gradually shortened.
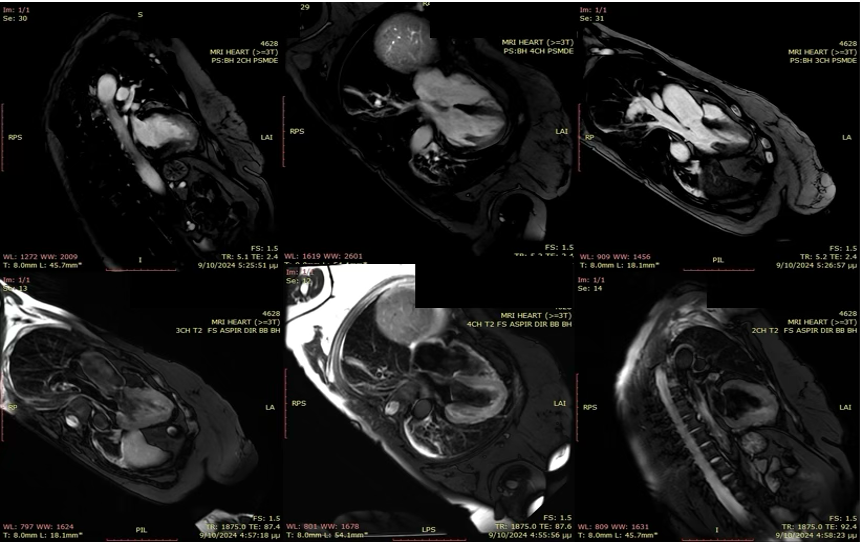
On day 20, CMR was performed, which confirmed impaired LV function with hypokinesis of the apical segments and an EF of 45%. There were no signs of myocardial infarction or fibrosis. It also showed diffuse oedema in the apical and mid planes (figure 4). The oedema in association with hypokinesis or akinesis in these segments is typical of Takotsubo cardiomyopathy (TTC). Moreover, the absence of delayed enhancement differentiates TTC from an ACS and acute myocarditis.
She had a prolonged recovery with a total of 60 days of hospitalisation. Her LV function gradually improved with some remaining apical hypokinetic segments. Despite addressing all reversible causes of sudden cardiac death during her hospitalisation, her LVEF remained mildly reduced and QT interval prolonged. After consultation with our electrophysiologists, we decided to place an ICD for secondary prevention of sudden cardiac death.
Discussion
Takotsubo cardiomyopathy (TTC) shares several features with ACS, including similar clinical presentation, ECG changes and elevated biomarkers of myocardial injury. It is very challenging to distinguish between them in the acute phase. The InterTak Diagnostic Score is a tool developed to aid in differential diagnosis.1 Additionally, TTC and ACS also share common pathophysiology; there is enhanced systemic inflammatory activation, elevated plasma catecholamines and underlying microvascular dysfunction in both syndromes. Both cardiac troponins (cTn) and natriuretic peptides (NPs) are increased in TTC and ACS. However, cTn and NPs levels are usually higher in ACS than TTC, especially if cTn is ≥26 times the upper limit of normal — this would be a powerful indicator of an ACS.2 An ECG in the case of TTC is sometimes confusing, as it is similar to that of an ACS (ST-segment repolarisation abnormalities can be found in both syndromes). In TTC, T-wave inversion on the ECG predicts a higher long-term mortality rate than in ACS.3 To discriminate between them, especially in the case of elevated cTn, CAG should be performed. In our case, CAG revealed moderate to severe stenosis in the middle part of the LAD coronary artery. Even though we already had echocardiographic evidence of TTS, the patient’s ongoing angina and gradually elevated cTn levels compelled interventional cardiologists to proceed to perform coronary angioplasty.
In the subacute phase, myocardial oedema occurs. Although not the direct aetiology of TTC, it may occur due to coronary spasm, catecholamine-mediated myocardial stunning and microvascular dysfunction. In CMR, the absence of late gadolinium enhancement (LGE) is a typical feature of TTC; however, recent studies have revealed the presence of LGE in some patients with TTC.4 Oedema might be reflected by negative T waves and QTc prolongation on ECG. In TTC, the QTc is prolongated because of reduced repolarisation reserve and intracellular overload secondary to transient myocardial insult.5 When combined with electrolyte imbalances, such as hypokalaemia and hypomagnesaemia, it could possibly lead to polymorphic ventricular tachycardia (VT). Pharmacologically induced bradycardia, especially with the usage of beta blockers, further prolongs the QTc interval.
In patients with TTC and VAs, the implantation of an ICD remains controversial. Some experts suggest the utilisation of a wearable defibrillator in patients with high-risk features.6 Moreover, in patients with TTS presenting with life-threatening VAs or cardiogenic shock, ICD implantation should be considered.7 In our case, with ACS conjoined, ICD therapy is recommended for secondary prevention of sudden cardiac death, as for patients who survived VF or with haemodynamically unstable VT, or VT with syncope and who have an LVEF ≤40%, who are receiving chronic optimal medical therapy, and who have a reasonable expectation of survival with good functional status for more than one year.8
Key messages
- TTS is usually benign, but it can sometimes lead to life threatening arrhythmias
- Coronary artery disease and TTS can co-exist
- In patients with TTS presenting with life-threatening VAs or cardiogenic shock, ICD implantation should be considered
Authorship
Surgical and medical practices: EO, AP, IT, SD, DG; concept: EO, DG; data collection or processing: EO; analysis or interpretation: EO, AP, DG; literature search: EO, AP; writing: EO, AP.
Acknowledgements
Dr Adam Graham, Consultant Cardiologist
Conflicts of interest
None declared.
Funding
None.
Statement of consent
Informed consent was obtained from the patient.
References
1. Yalta K, Madias JE, Kounis NG et al. Takotsubo syndrome: an international expert consensus report on practical challenges and specific conditions (part 1: diagnostic and therapeutic challenges). Balkan Med J 2024;41:421–41. https://doi.org/10.4274/balkanmedj.galenos.2024.2024-9-98
2. Couch LS, Garrard JW, Henry JA et al. Comparison of troponin and natriuretic peptides in Takotsubo syndrome and acute coronary syndrome: a meta-analysis. Open Heart 2024;11:e002607. https://doi.org/10.1136/openhrt-2024-002607
3. Gietzen T, El-Battrawy I, Lang S et al. Impact of T-inversion on the outcome of Takotsubo syndrome as compared to acute coronary syndrome. Eur J Clin Invest 2019;49:e13078. https://doi.org/10.1111/eci.13078
4. Kato K, Daimon M, Sano M et al. Dynamic trend of myocardial edema in Takotsubo syndrome: a serial cardiac magnetic resonance study. J Clin Med 2022;11:987. https://doi.org/10.3390/jcm11040987
5. Takasaki A, Nakamori S, Dohi K. Massive ST-segment elevation and QTc prolongation in the emergency department. Circulation 2019;140:436–9. https://doi.org/10.1161/CIRCULATIONAHA.119.041736
6. El-Battrawy I, Erath JW, Lang S et al. Takotsubo syndrome and cardiac implantable electronic device therapy. Sci Rep 2019;9:16559. https://doi.org/10.1038/s41598-019-52929-5
7. Singh T, Khan H, Gamble DT, Scally C, Newby DE, Dawson D. Takotsubo syndrome: pathophysiology, emerging concepts, and clinical implications. Circulation 2022;145:1002–19. https://doi.org/10.1161/CIRCULATIONAHA.121.055854
8. Kusumoto FM, Calkins H, Boehmer J et al. HRS/ACC/AHA expert consensus statement on the use of implantable cardioverter-defibrillator therapy in patients who are not included or not well represented in clinical trials. J Am Coll Cardiol 2014;64:1143–77. https://doi.org/10.1016/j.jacc.2014.04.008
