Conventional management of out-of-hospital cardiac arrest (OOHCA) in patients with unusual cardiac anatomy may result in inferior outcomes. It is important that appropriate consideration of these patients is made when developing OOHCA resuscitation guidelines. Initiatives to improve outcomes following OOHCA, such as community training of resuscitation techniques, should take patients with unusual cardiac anatomy into account. We present a male in his twenties with heterotaxy syndrome, a congenital defect with abnormally arranged intrathoracic and intra-abdominal organs. He experienced an unwitnessed OOHCA with a downtime of approximately 20 minutes. He had complex congenital heart disease and had undergone previous palliative cardiac surgery resulting in a Fontan circulation. Despite maximal inotropic and vasopressor support, he developed multi-organ failure with diffuse hypoxic brain injury warranting care withdrawal. In this case report we discuss the important roles of appropriate community resuscitation in patients with unusual cardiac anatomy and of mechanical circulatory support in patients with single ventricle physiology.

Introduction
Out-of-hospital cardiac arrest (OOHCA) is associated with high morbidity and mortality rates worldwide.1 Although there have been advances in the management of cardiac conditions, because OOHCA occurs in the community with lack of access to immediate and effective cardiopulmonary resuscitation (CPR), OOHCA has continued to yield poor clinical outcomes globally.1,2 Several interventions have been developed to improve effective CPR for OOHCA patients,2,3 one of which is community training of CPR techniques.
In patients with unusual cardiac anatomy, modified CPR techniques need to be adopted, and this has not been considered in the community training of CPR. Standard CPR is not as effective in these patients and leads to even poorer outcomes following OOHCA.1 In the United Kingdom (UK), the National Institute of Health, and Care Excellence (NICE) guidelines for CPR in patients with OOHCA4 have failed to consider CPR in patients with unusual cardiac anatomy.
In this case report, we discuss the challenges and complexities associated with the management of a patient with heterotaxy syndrome (HS; situs ambiguous), with single ventricle physiology and palliated with a Fontan procedure who presented following an OOHCA.
Case
A male patient in his twenties presented following an unwitnessed OOHCA and was found unconscious by a family member who commenced bystander CPR. When the emergency response team arrived, CPR was continued. He was found to have a ventricular tachycardia (VT) and was subsequently cardioverted, after which he then developed ventricular fibrillation (VF) requiring further cardioversion to achieve sinus rhythm. He received four doses of 1 mg intravenous adrenaline and had a total downtime of approximately 20 minutes prior to recovery of spontaneous circulation (ROSC).
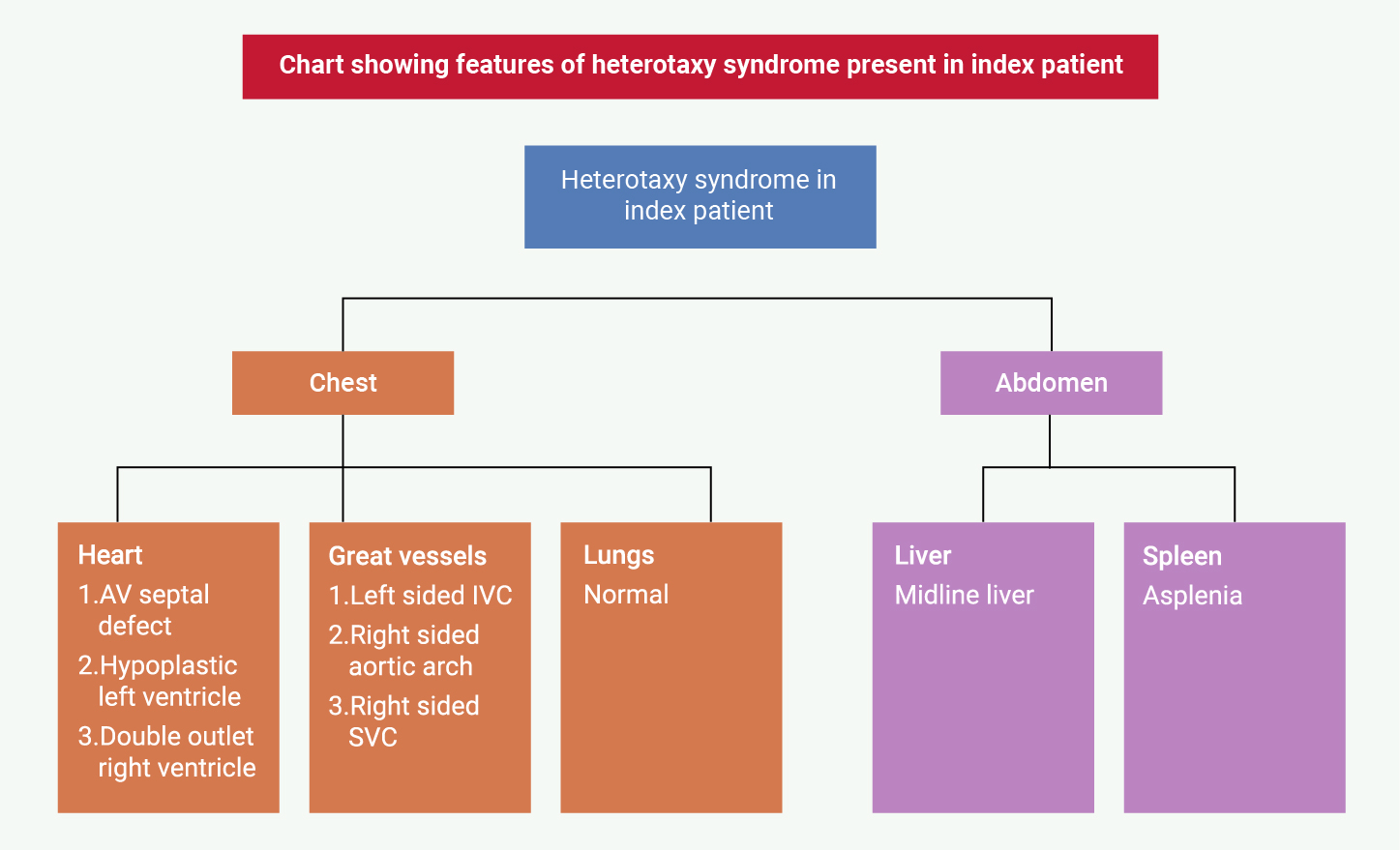
Prior to this event, he had no immediate complaints. He had a significant cardiac medical history with a known history of HS with right atrial isomerism, transposition of the great arteries and levocardia. He had an unbalanced atrioventricular septal defect with a hypoplastic left ventricle and a double outlet right ventricle (functionally a single ventricle physiology). He had a midline liver, a left-sided inferior vena cava (IVC), asplenia, a single right superior vena cava and a right-sided aortic arch (figure 1).
He had several previous cardiac interventions with pulmonary artery banding as an infant, bidirectional cavo-pulmonary connection (Glenn procedure) at the age of three, and a total cavo-pulmonary connection (TCPC, Fontan procedure) with an extracardiac conduit at the age of 12. He had a single episode of syncope requiring CPR at the age of 20 with no subsequent arrhythmias identified on implantable loop recorder. Other medical history included factor V Leiden deficiency and Fontan-associated liver disease. Prior magnetic resonance imaging and echocardiography performed at his latest follow-up appointment showed severe atrioventricular valve regurgitation, dynamic muscular systemic outflow obstruction and moderate narrowing of the IVC at the anastomosis with the extracardiac conduit. Intervention had been considered within the adult congenital heart disease (ACHD) surgical centre; however, it was considered high risk and not currently indicated due to the patient being largely asymptomatic with preserved performance on cardiopulmonary exercise testing.
On arrival to the intensive care unit (ICU) following helicopter retrieval, he had a Glasgow coma scale (GCS) score of 3/15 and was immediately intubated. Post-cardiac arrest management was initiated for neuroprotection. Generalised low-amplitude jerky movements were noted and levetiracetam was commenced. He was haemodynamically stable but a strategy for mechanical circulatory support (MCS) was considered, should cardiogenic shock develop.
Four hours following presentation, he had a sudden loss of cardiac output with a supraventricular tachycardia (SVT) requiring cardioversion to sinus rhythm and addition of vasopressor and inotropic support. He was also noted to have had a single episode of large-volume melaena. Urgent computed tomography (CT) scan of the chest, abdomen, and pelvis showed bowel dilatation without obstruction, and no proximal pulmonary embolus (PE). A CT brain demonstrated no acute intracranial pathology. Further episodes of large-volume melaena associated with oliguria occurred at 10-hours post-admission. He was commenced on continuous veno-venous hemofiltration (CVVH).
Despite maximum vasopressor and inotropic support, he slowly developed worsening multi-organ failure with acute kidney injury, acute liver injury, poor neurological response (absence of corneal or cough reflex, sluggish pupils and no motor/verbal or eye-opening responses off sedation), myoclonic jerks, ongoing gastrointestinal bleeding and worsening metabolic acidosis. A repeat CT head on day two showed severe hypoxic ischaemic encephalopathy with trans-tentorial herniation. A CT thorax showed a new PE at the bifurcation of the left main pulmonary artery into its lobar branches, while a CT abdomen and pelvis showed ileal and colonic oedema consistent with enterocolitis. Given the diagnosis of severe hypoxic brain injury, life support was withdrawn on day four following a multi-disciplinary team and family discussion.
Discussion
Right atrial isomerism is a subtype of HS and is a rare congenital abnormality occurring in less than 1% of patients with congenital heart disease.5 It occurs when paired structures on the left side are morphological mirror images of the right-sided structures. Abnormalities include a midline liver, asplenia, bilateral tri-lobed lungs and situs inversus of intrathoraco-abdominal organs, including the heart and great vessels.5,6 The Fontan procedure is a surgical procedure that involves the diversion of venous blood directly to the pulmonary artery, bypassing the right side of the heart.7 This procedure is indicated in patients with anatomy where septation of the heart is not possible, and in single ventricle physiology such as in hypoplastic left or right heart syndrome.
One study investigated the optimal CPR positioning of patients with a single ventricle who have had the Fontan procedure. The authors concluded that in Fontan patients, the ideal area of chest compression during CPR is 5–25% below the mid-sternum.8 This area is much lower than the mid-sternum recommended for standard CPR in the general population. The lack of modification to the chest compression site might have contributed to potential ineffectiveness and neurological complications. With increasing life expectancy of patients with ACHD,9 it is important that the modified CPR techniques for this group of patients are incorporated into the CPR community training programmes and into the adult resuscitation guidelines to provide them with the best chance of survival.
However, it is important to acknowledge that bystander CPR is designed to be simple to ensure quick and confident action of bystanders. Thus, adapting CPR techniques for special populations like Fontan patients can confuse lay individuals and lead to hesitation or inaction, which increases risk. While widespread public CPR training cannot reasonably be expected to incorporate nuanced exceptions for rare pathologies, an important compromise is to specifically train caregivers, teachers and family members of Fontan patients on these modified techniques. In addition, advance care planning and the use of medical alert systems or care cards that may assist first responders in these patients are important.
Currently, there are limited guidelines for CPR management in adult patients with abnormal cardiac anatomy. In 2018, the American Heart Association produced the CPR guidelines for paediatric patients with cardiac diseases in view of the need for modified CPR in patients with abnormal cardiac anatomy.10 There was, however, no modified guideline for chest compressions during CPR for patients with ACHD. In the recent 2021 guidelines by the Resuscitation Council UK (RCUK), there is no discussion around resuscitation management for patients with unusual cardiac anatomy or ACHD.11 In the paediatric basic and advanced life support guidelines by the RCUK, they note special circumstances including single ventricle and Fontan physiology. They recommend conventional CPR but suggest ventilatory modifications, such as permissive hypercarbia or use of negative pressure ventilation in hemi-Fontan/Fontan states, and early consideration of extracorporeal CPR in refractory arrest.11,12 In the adult guidelines, there are no separate guidelines for Fontan patients.13
A joint working group of the British Cardiovascular Society, British Congenital Cardiac Association and British Cardiovascular Intervention Society, in discussion with the Grown-Up Congenital Heart Patients Association, produced the UK national congenital heart policy guidelines in patients with congenital heart disease. The guidelines provide clinical guidelines covering congenital heart disease care patterns, although CPR-specific protocols are less directly addressed. They recommended that patients with Fontan circulation are managed under the standard adult advanced life support (ALS) algorithm — with physiological awareness rather than bespoke modifications.14
The UK national initiatives to improve outcomes following OOHCA did not incorporate consideration for these groups of patients3 and guidelines need to be updated to take them into account. The UK national initiative to increase and improve CPR training in the community needs to be updated to include teaching of modified CPR techniques to target patients with abnormal cardiac anatomy. With a prevalence of congenital heart disease of 8 in 1,000 live births in the UK and increased survival of these patients to adulthood, adequate measures need to be taken to ensure that no area of management in these patients is marginalised.15 It is also important to provide an awareness to the public on the peculiar physiology of patients with unusual physiology that may require modified CPR in the community. Bystander CPR favours chest compressions over ventilation, however, early ventilation is more important in Fontan patients.
Modification of in-hospital CPR due to the altered physiology in Fontan patients has been suggested in addition to the position of chest compression. These includes early initiation of ventilation, use of high-flow oxygen, aggressive preload support (with judicious use of fluids), cautious addition of vasopressors, abdominal compressions in paediatric patients, and early extracorporeal CPR in centres with extracorporeal membrane oxygenation (ECMO) capabilities.16–18 The only modification relevant to bystander out-of-hospital CPR is the modification of chest compression position, which is why that was the emphasis of our discussion.
Further possible adaptations to chest compression in patients with Fontan circulation has been reported in paediatric patients e.g., right-sided compressions in dextrocardia or posterior–anterior compressions in patients with a more posteriorly located ventricle.19 These modifications have not been reported in the adult population.
We also reviewed the North American (AHA/ILCOR) guidelines and although there was mention of necessary awareness of Fontan physiology, the CPR algorithm remained unchanged. The European Resuscitation Council (ERC) guidelines, while also acknowledging Fontan patients as special, provided no dedicated section or tailored recommendations for CPR. From our search, no congenital heart society guidelines include Fontan CPR modification suggestions. Guideline recommendations are usually based on adequately powered research studies and the lack of literature to support improved outcomes using CPR modification is likely to serve to deter inclusion in resuscitation guidelines. This may be exacerbated by the fact that the Fontan population make up a very small proportion of the entire CPR population.
Post-resuscitation care
There are also limited guidelines for post-resuscitation care following OOHCA in this patient group. One area of important consideration in these patients is the feasibility of MCS. Following OOHCA, multi-organ protection is very important to ensure adequate reperfusion to vital organs after a period of global ischaemia during cardiac arrest.20 In patients with HS or Fontan patients, special consideration needs to be given to the planning of temporary MCS in emergency situations.21,22 There have been a few successful case reports on the use of MCS including ventricular assist devices (VAD) and ECMO for paediatric patients with functional single ventricle heart failure following the Fontan procedure as a bridge to heart transplantation.22–24 However, with the lack of large-volume research, not much is known about the overall effectiveness of MCS in these patients.
The presence of a functional morphologic right ventricle can serve as a limitation to the use of a VAD for MCS. In a failing morphological right ventricle, the relatively thinner right wall compared to the left makes cannulation of the inflow cannula difficult.22 Furthermore, the position of the apex, which is not completely oriented inferiorly, could cause inflow obstruction.21 Also, the remodelling of the atria (atrial wall thickening and dilation) following the Fontan procedure leads to haemodynamic changes, typically right atrial hypertension.25 Conventional MCS for right-sided heart failure cannot be achieved with a right-sided VAD in Fontan patients due to the absence of the right ventricle.
Establishing veno-arterial (VA) or veno-venous (VV) ECMO circulation in the paediatric age group via the carotid artery and right jugular vein has been described in Fontan patients.22 In older paediatric patients, the use of femoral artery and femoral vein as an alternative has been established.22 However, in our patient, the presence of heterotaxy would need to be taken into consideration. There have been reports of successful use of short-term MCS as a bridge to transplant or recovery in patients with heterotaxy. Rajab et al reported VV ECMO cannulation as a bridge to heart–lung transplantation in a patient with dextrocardia.26 Zhang et al also reported a case of central VA ECMO in a patient with dextrocardia and cardiogenic shock following off-pump coronary bypass graft surgery.27 Further to this, there are emerging MCS solutions for the right side, such as Impella RP (Abiomed, Danvers, MA, USA)28 and EXCOR Venous Cannula (Berlin Heart GmbH, Berlin, Germany)29 in patients with a failing Fontan circulation.
The timing of initiating MCS is also an area that has been poorly explored even though optimal timing is important. Studies have shown that prompt initiation of MCS in patients for which it is indicated can double survival.21 Thus, in patients with a failing Fontan circulation, the decision for MCS must be prompt and timely.
Patients with late Fontan failure can present either with impaired or preserved systemic ventricular function as an indication for MCS.22 In our patient, there was no indication for MCS as his haemodynamic parameters were reasonable (apart from raised right-sided Fontan pressures) and depended on his potential for neurological recovery.
Key messages
- The management of out-of-hospital cardiac arrest in patients with unusual cardiac anatomy is unique and differs from conventional cardiopulmonary resuscitation (CPR)
- There is a need for resuscitation guidelines to incorporate modified CPR techniques for patients with adult congenital heart disease (ACHD)
- Initiatives to educate community members on CPR should take this group of patients into consideration
- Mechanical circulatory support in ACHD patients can be challenging and strategies for support should be individualised and planned for, when required
Acknowledgements/Authorship
Dr Oluwanifemi Akintoye: Conceptualisation, design, drafting, final approval of submitted version.
Dr Clive Lewis: Conceptualisation, design, draft review, final approval of submitted version.
Conflicts of interest
None declared.
Funding
A £300 research grant approved by the Royal Papworth Hospital Charity to support publication of this case report.
Statement of consent and ethical approval
Ethical approval was not required for this case report as there is no publication of identifiable patient data. The patient’s next of kin was contacted for consent and has signed an informed consent form agreeing to the publication of this case report. The consent form can be made available upon requested.
References
1. Yan S, Gan Y, Jiang N et al. The global survival rate among adult out-of-hospital cardiac arrest patients who received cardiopulmonary resuscitation: a systematic review and meta-analysis. Crit Care 2020;24:61. https://doi.org/10.1186/s13054-020-2773-2
2. Brooks SC, Clegg GR, Bray J et al. Optimizing outcomes after out-of-hospital cardiac arrest with innovative approaches to public-access defibrillation: a scientific statement from the International Liaison Committee on Resuscitation. Circulation 2022;145:e776–801. https://doi.org/10.1161/CIR.0000000000001013
3. Perkins GD, Lockey AS, Belder MA de, Moore F, Weissberg P, Gray H. National initiatives to improve outcomes from out-of-hospital cardiac arrest in England. Emerg Med J 2016;33:448–51. https://doi.org/10.1136/emermed-2015-204847
4. NICE. Cardiac arrest – out of hospital care. Last revised January 2024. Available from: https://cks.nice.org.uk/topics/cardiac-arrest-out-of-hospital-care/
5. Yang L, Zhou L, Chen L. Right atrial isomerism diagnosed by STIC-HD live flow and autopsy: a case report. Medicine 2021;100:e24912. https://doi.org/10.1097/MD.0000000000024912
6. Eitler K, Bibok A, Telkes G. Situs inversus totalis: a clinical review. Int J Gen Med 2022;15:2437–49. https://doi.org/10.2147/IJGM.S295444
7. Lee M, Alahmadi MH, Shahjehan RD. Fontan Completion. [Updated 19 January 2025] In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK558950/
8. Park JB, Song IK, Lee JH, Kim EH, Kim HS, Kim JT. Optimal chest compression position for patients with a single ventricle during cardiopulmonary resuscitation. Pediatr Crit Care Med 2016;17:303–6. https://doi.org/10.1097/PCC.0000000000000658
9. Reid GJ, Webb GD, Barzel M, McCrindle BW, Irvine MJ, Siu SC. Estimates of life expectancy by adolescents and young adults with congenital heart disease. J Am Coll Cardiol 2006;48:349–55. https://doi.org/10.1016/j.jacc.2006.03.041
10. Marino BS, Tabbutt S, MacLaren G et al. Cardiopulmonary resuscitation in infants and children with cardiac disease: a scientific statement from the American Heart Association. Circulation 2018;137:e691–782. https://doi.org/10.1161/CIR.0000000000000524
11. Resuscitation Council UK. Special circumstances guidelines. 2021. Available from: https://www.resus.org.uk/library/2021-resuscitation-guidelines/special-circumstances-guidelines
12. Paediatric advanced life support Guidelines | Resuscitation Council UK [Internet]. [cited 2025 Aug 2]. Available from: https://www.resus.org.uk/library/2021-resuscitation-guidelines/paediatric-advanced-life-support-guidelines
13. Adult advanced life support Guidelines | Resuscitation Council UK [Internet]. [cited 2025 Aug 2]. Available from: https://www.resus.org.uk/library/2021-resuscitation-guidelines/adult-advanced-life-support-guidelines
14. NHS England. Congenital Heart Disease and Paediatric Cardiac Clinical Network Specification. 2023. Available from: https://www.england.nhs.uk/wp-content/uploads/2024/05/PRN231104-chd-paediatric-cardiac-network-specification-2023-.pdf
15. NCHDA-Domain-Report_2021_FINAL.pdf [Internet]. [cited 2023 Sep 6]. Available from: https://www.nicor.org.uk/wp-content/uploads/2021/10/NCHDA-Domain-Report_2021_FINAL.pdf
16. Sperotto F, Gearhart A, Hoskote A et al. Cardiac arrest and cardiopulmonary resuscitation in pediatric patients with cardiac disease: a narrative review. Eur J Pediatr 2023;182:4289–308. https://doi.org/10.1007/s00431-023-05055-4
17. Yates AR, Hehir DA, Reeder RW et al. Resuscitation arterial waveform quantification and outcomes in pediatric bidirectional Glenn and Fontan patients. Pediatr Res 2025;97:1989–96. https://doi.org/10.1007/s00431-023-05055-4
18. Tewari P, Babu SG. Resuscitation after modified Fontan procedure. Ann Thorac Surg 1994;58:880–2. https://doi.org/10.1016/0003-4975(94)90775-7
19. Kim JH, Jung JY, Lee S et al. Ideal chest compression site for cardiopulmonary resuscitation in Fontan circulation patients with dextrocardia. BMC Cardiovasc Disord 2024;24:22. https://doi.org/10.1186/s12872-023-03691-0
20. Mongardon N, Dumas F, Ricome S et al. Postcardiac arrest syndrome: from immediate resuscitation to long-term outcome. Ann Intensive Care 2011;1:45. https://doi.org/10.1186/2110-5820-1-45
21. Woods RK, Ghanayem NS, Mitchell ME, Kindel S, Niebler RA. Mechanical circulatory support of the Fontan patient. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu 2017;20:20–7. https://doi.org/10.1053/j.pcsu.2016.09.009
22. Mascio CE. Mechanical support of the failing Fontan circulation. Semin Thorac Cardiovasc Surg 2021;33:454–8. https://doi.org/10.1053/j.semtcvs.2020.09.005
23. Morales DLS, Adachi I, Heinle JS, Fraser CD. A new era: use of an intracorporeal systemic ventricular assist device to support a patient with a failing Fontan circulation. J Thorac Cardiovasc Surg 2011;142:e138–40. https://doi.org/10.1016/j.jtcvs.2011.05.018
24. Rossano JW, Woods RK, Berger S et al. Mechanical support as failure intervention in patients with cavopulmonary shunts (MFICS): rationale and aims of a new registry of mechanical circulatory support in single ventricle patients. Congenit Heart Dis 2013;8:182–6. https://doi.org/10.1111/chd.12053
25. Wolf CM, Seslar SP, den Boer K et al. Atrial remodeling after the Fontan operation. Am J Cardiol 2009;104:1737–42. https://doi.org/10.1016/j.amjcard.2009.07.061
26. Rajab TK, Kim T, Keller S, Mallidi H. Management of a young patient with dextrocardia, atrial septal defect, and Eisenmenger syndrome with venous-venous extracorporeal membrane oxygenation and heart-lung transplantation. J Card Surg 2019;34:1114–6. https://doi.org/10.1111/jocs.14168
27. Zhang X, Wang P, Fu Z et al. Application of ECMO in a patient with post-cardiotomy cardiogenic shock combined with dextrocardia: case report. 2022. Available at: https://doi.org/10.21203/rs.3.rs-2348123/v1
28. Saef J, Montgomery R, Cedars A et al. Durable mechanical circulatory support in adult congenital heart disease: reviewing clinical considerations and experience. J Clin Med 2022;11:3200. https://doi.org/10.3390/jcm11113200
29. Karner B, Urganci E, Schlein J et al. First-in-man use of the EXCOR Venous Cannula for combined cavopulmonary and systemic ventricular support in Fontan circulation failure. J Heart Lung Transplant 2022;41:1533–6. https://doi.org/10.1016/j.healun.2022.06.009
