Sonographer- and nurse-led clinics were developed at a cardiothoracic centre and a sonographer-led clinic at a district general hospital (DGH). Common database fields were adopted in 2007 and this is an audit over the subsequent two years. Data were analysed for the two-year period from 1 September 2007 to 31 August 2009. A total of 683 visits by 388 patients occurred at the cardiothoracic centre and 1,306 visits by 726 patients at the DGH. There were no unexpected adverse events. Cross-referral to a cardiologist occurred in 13% of visits at the cardiac centre and 11.5% at the DGH. The mortality rates were 2% and 3%, the discharge rates 6% and 2%, and the surgical rates 16% and 4% at the cardiac centre and the DGH, respectively. No unexpected events occurred.
Our observations suggest that devolved surveillance clinics are feasible, safe and generalisable as part of a specialist valve service.
Introduction
Valve disease, is increasingly common as our population ages.1 The organisation of care for these patients is patchy,2 while judging the suitability, timing and type of intervention has never been harder. Opinion papers, therefore, call for a cardiologist specialising in valve disease at every major hospital.3,4 However, patients with valve disease often remain asymptomatic for a long period and need regular echocardiography, but not necessarily to see a cardiologist. Such patients can be managed in a sonographer-led clinic, while patients with normally functioning mechanical replacement valves who do not require regular echocardiography can be managed in a nurse-led clinic. We developed specialist valve clinics with devolved surveillance independently at a cardiac centre at Guy’s and St Thomas’ Hospitals (GSTT) and at Eastbourne district general hospital (DGH). The inclusion criteria were: asymptomatic moderate and severe native valve disease; replacement heart valve; mitral valve repair; bacteriologically cured infective endocarditis; aortic dilatation. Patients were excluded for co-existing conditions requiring medical opinion. The clinic structure including protocols is described in detail elsewhere.5,6 Common echocardiographic thresholds derived from International guidelines7,8 and database fields were adopted in 2007, with the exception of patients with mechanical replacement heart valves who had annual echocardiograms at the DGH but not GSTT. This report describes an audit for the two years between 1 September 2007 and 31 August 2009.
Results of the two-year audit
There were 683 clinic visits by 388 patients at GSTT and 1,306 visits by 726 patients at the DGH. The median age of the patients was 65.5 (range 16–93) years at GSTT and 73 (range 20–91) years at the DGH. At the two clinics there were a total of 358 visits primarily to the cardiologist and 1,631 to the devolved clinics. However, the cardiologist needed to see 43 (13%) of the 325 patients initially seen by the nurse or sonographer at GSTT and 150 (11.5%) from the sonographer-led clinic in the DGH. The main reasons were a change in symptoms, a clinical event, or the attainment of an echocardiographic threshold. This, therefore, represents a net saving of 1,438 visits to a cardiologist. Discharge resulted from 42 (6%) visits at GSTT and 19 (2%) visits at the DGH. The main reasons were because the valve disease was only mild, or the patient preferred local follow-up, or was too frail to re-attend. Deaths occurred in seven patients (2%) at GSTT, all after aortic valve replacement or from nonvalve causes. There were 23 (3%) deaths at the DGH, three from progressive valve disease (two not suitable for transcatheter valve implantation [TAVI], and one referred for TAVI but died before this could be performed), two from heart failure (both with inoperable functional mitral regurgitation), and the rest from nonvalve causes. At GSTT, 61 patients (16%) had an intervention, 53 conventional surgery and eight TAVI. In the DGH, 28 (4%) had surgery of whom five were referred directly from the clinic without seeing a cardiologist. There were no adverse valve-related events in patients followed in sonographer- or nurse-led clinics. One patient from the sonographer-led clinic was admitted because of type II respiratory failure.
At the DGH, 90 patients with mechanical replacement valves had echocardiograms, 55 in the aortic, 34 in the mitral and one in both positions. In only one case was a postoperative echocardiogram available in the surgical discharge summary. There were 15 clinical events. In a further two aortic replacements, echocardiography showed a rise in gradient judged to be within normal limits after subsequent investigation. Therefore, the yield from routine follow-up echocardiography was zero in the absence of clinical indications.
Discussion
The main advantage of a specialist clinic is to deliver higher quality care than in a general clinic as a result of greater volumes allied to specialisation of training, continuing education and clinical interest. Guidelines are more consistently applied9 and the number of inappropriate echocardiograms reduced.9 This audit confirms that routine echocardiography for normally functioning mechanical replacement valves is not necessary.7,8
Devolving surveillance to sonographer or nurse within the clinic structure frees the cardiologist to see those patients requiring clinical decisions, and our experience is that this is safe. The clinics are popular with patients who enjoy continuity of care, reduced waiting times, the ‘one-stop’ service, and flexibility of appointments. Sonographers or nurses seeing patients in the place of registrars saves costs and releases the registrar for training or other clinical duties. The clinics have also been useful for training nurses and medical students in auscultation, and registrars in the management of valve disease. Some of the roles are interchangeable so that our sonographer-led clinics could equally be run by a nurse undertaking the clinical evaluation with a sonographer purely for the echocardiography. We, therefore, expect that elements of these two models should be generalisable to any hospital. However, there are important provisos:
The clinic sonographers and nurses are experienced and highly qualified. We ensured appropriate training before starting the clinics and confirmed clinical assessment. A devolved clinic would not necessarily be safe with more junior staff.
More cases than anticipated, about 12%, required advice from a cardiologist. Ideally, this needs to be within the same clinic. The principle operational difficulty at the DGH was communication with and referral back to the general cardiology out-patient clinics, which were too full to allow early review.
A surveillance clinic appointment is 60 minutes long allowing for scanning, the clinical assessment and administration. This is longer than the 45-minute standard echocardiography appointment. Furthermore, both clinics have expanded since their inception resulting in strains in other areas of the echocardiography departments.
Some patients stayed within the clinic despite being unsuitable for conventional or transcatheter procedures either because of advanced old age or comorbidity. These patients remained appropriate for the consultant-supervised clinic at the centre, but criteria for discharge from a sonographer-led clinic would need to be agreed at the outset.
Clear communication between the surgical centre (hub) and the district centre (spoke) is essential, particularly the dissemination of operation notes and postoperative echocardiography report.
Conclusion
Valve disease is often managed in general clinics by cardiologists whose primary interest lies elsewhere. We suggest, instead, that there should be specialist multi-disciplinary valve clinics in a ‘hub-and-spoke’ arrangement.5 At the ‘hub’ is a cardiologist-supervised clinic in a cardiothoracic centre with ‘spokes’ represented by a devolved specialist surveillance clinic at a district hospital or, potentially, in the community. Devolving surveillance to a sonographer or nurse as part of a specialist valve service is feasible, safe and generalisable, and allows the cardiologist to spend more time making clinical decisions.
Acknowledgements
We thank Dr Ravi Rayasam and Ms Lesley Hart for their invaluable help in the preparation of this manuscript.
Conflict of interest
None declared.
Key messages
Valve disease is often managed in general clinics by cardiologists whose primary interest lies elsewhere
The main advantage of a specialist clinic is to deliver higher quality care than in a general clinic
Devolved surveillance clinics are feasible, safe and generalisable as part of a specialist valve service
References
Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. Lancet 2006;368:1005–11. (doi: 10.1016/S0140-6736(06)69208-8)
Iung B, Baron G, Butchart EG et al. A prospective survey of patients with valvular heart disease in Europe: the Euro Heart Survey on valvular heart disease. Eur Heart J 2003;24:1231–43. (doi: 10.1016/S0195-668X(03)00201-X)
Bridgewater B, Hooper T, Munsch C et al. Mitral repair best practice: proposed standards. Heart 2006;92:939–44. (doi: 10.1136/hrt.2005.076109)
Chambers J. Aortic stenosis is common but often unrecognised. BMJ 2005;330:801–02.
Chambers JB, Lloyd G, Rimington HM et al. The case for a multidisciplinary specialist valve clinic. J Heart Valve Disease (in press).
Valve Study Group. www.researchechocardiography.com
Vahanian A, Baumgartner H, Bax J et al. Guidelines on the management of valvular heart disease. Eur Heart J 2007;28:230–68. (doi: 10.1093/eurheartj/ehm095)
Bonow RO, Carabello BA, Chatterjee K et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease. J Am Coll Cardiol 2006;48:e1–e148. (doi: 10.1016/j.jacc.2006.05.021)
Taggu W, Topham A, Hart L et al. A cardiac sonographer led follow up clinic for heart valve disease. Int J Cardiol 2009;132:240–3. (doi: 10.1016/j.ijcard.2007.11.076)
Alcohol septal ablation (ASA) is an alternative therapeutic method to the gold-standard surgical myectomy in the treatment of symptomatic left ventricular outflow tract (LVOT) obstruction in patients with hypertrophic cardiomyopathy (HCM). ASA is performed by injecting alcohol into the target septal branch of the left anterior descending coronary artery. In this article, we review the rationale and indications for ASA, provide a practical description of the technique and give an overview of the published data placing it in context with the surgical approach. We also report our experience of the technique in a typical sample of patients referred to a tertiary centre providing demographic, echocardiographic and clinical outcomes data during an average follow-up period of three years. Our data confirm that ASA is an effective non-surgical technique for treatment of symptoms related to LVOT obstruction in HCM. Medium-term follow-up demonstrates persistent reduction in LVOT obstruction and improvement in New York Heart Association (NYHA) functional class. Long-term studies of larger populations are necessary to determine the wider prognostic significance of the procedure.
Introduction
Hypertrophic cardiomyopathy (HCM) is an inherited cardiac muscle disorder, transmitted predominantly in an autosomal dominant fashion with variable penetrance and an estimated prevalence of one in 500 in the western population.1 Myocardial hypertrophy most commonly affects the interventricular septum and may be associated with dynamic obstruction of the left ventricular outflow tract (LVOT),2 caused by systolic anterior motion (SAM) of the mitral valve leaflets. LVOT obstruction may occur at rest or only become apparent during physiological stress. Symptoms related to LVOT obstruction include dyspnoea, exertional chest pain, pre-syncope or syncope. Conventional medical treatment for symptoms related to outflow obstruction includes beta blockers, calcium channel antagonists, and occasionally disopyramide. Dual-chamber pacemaker implantation has also been shown to have some symptomatic benefit, although blinded crossover studies suggested this benefit was limited to elderly patients.3 Surgical myectomy has been established as the primary treatment modality to relieve outflow tract obstruction associated with severe drug-refractory heart failure symptoms and marked functional disability (New York Heart Association [NYHA] class III/IV).
Alcohol septal ablation (ASA), first reported in 1995 by Sigwart,4 is an alternative therapeutic method to surgical myectomy for the treatment of LVOT obstruction. ASA is performed by injection of absolute alcohol into the septal branch of the left anterior descending (LAD) coronary artery producing a ‘therapeutic infarction’ within the basal ventricular septum. The localised myocardial necrosis leads to progressive scarring and a subsequent thinning of the basal septal region, expanding the LVOT. This reduces or eliminates SAM, ultimately leading to a reduction in sub-aortic obstruction4-6 and mitral regurgitation, mimicking the haemodynamic consequences of surgical septal myectomy.7,8 Similar outcomes in terms of improvement in symptoms and relief of LVOT obstruction have been reported for both ASA and surgical myectomy, although the incidence of permanent pacemaker implantation is generally greater after ASA.9,10
Indications for alcohol septal ablation
The American College of Cardiology and European Society of Cardiology (ACC/ESC) published joint guidance on the management of hypertrophic cardiomyopathy in 2003.11 The indications for ASA in these guidelines are widely accepted as follows: (a) severe heart failure symptoms (NYHA class III or IV) refractory to appropriate medical therapy, associated witha (b) sub-aortic gradient of 50 mmHg (peak) or greater, measured with Doppler echocardiography either at rest and/or during physiological exercise. The outflow gradients should either be secondary to SAM or proximal mitral valve-septal contact.
Technique
This section provides a descriptive account of the procedure as performed in our centre. All cases were performed via the femoral arterial approach such that a 6-French sheath was placed in the right femoral artery and 5-French sheath in the left side. In those without a permanent pacemaker (PPM), a 5-French venous sheath was also inserted to allow back-up temporary pacing of the right ventricle. Diagnostic coronary angiography was then performed to exclude significant coronary artery disease and to assess the septal branch as a potential target for alcohol ablation. A pigtail catheter was then advanced into the mid-cavity of the left ventricle for the measurement of intra-cavity pressure. A 6-French guide catheter was used to cannulate the left coronary artery and to obtain simultaneous aortic pressures to allow continuous assessment of the LVOT gradient. A long guidewire was then passed into the selected proximal septal branch and a separate guide wire placed into the LAD (figure 1A). An over-the-wire balloon was then inflated in the septal branch just beyond its origin to prevent the spillage of alcohol into the LAD. The guidewire in the septal branch was removed and contrast medium injected through the balloon lumen to delineate the area supplied by the septal branch and to ensure no retrograde flow into the LAD (figure 1B). In selected cases, myocardial contrast echocardiography (MCE) was performed, in order to echocardiographically delineate the myocardial territory supplied by the chosen septal branch (figure 2). This was followed by slow instillation of absolute alcohol (volume administered depending on the septal thickness and branch size) over two to five minutes. The LVOT gradient and electrocardiogram (ECG) were monitored continuously. The temporary wire was left in-situ for 24–48 hours post-procedure and patients were closely monitored for at least 48 hours. Serial measurements of cardiac enzymes (creatine kinase; CK) were made at 12, 24 and 48 hours post-procedure.
Figure 1. A. Separate guidewires are positioned in the left anterior descending (LAD) (a) and first septal branch (b). Also noted is a temporary pacing wire in the right ventricular apex (c), pigtail catheter (d) in the left ventricular cavity and guide catheter engaged in the left coronary artery (e). B. An over-the-wire balloon is then inflated in the septal branch and the guidewire removedFigure 2. Ultrasound contrast microbubbles injected into the septal branch are visualised echocardiographically (orange) in the apical four-chamber view and shown to perfuse the proximal septum confirming that the septal branch is supplying the target area for alcohol ablation
Manchester Heart Centre experience
The technique of ASA has been performed in our centre since January 2004. Patients were considered eligible for ASA in accordance with ACC/ESC guidelines. All patients underwent baseline clinical assessment, as well as transthoracic echocardiography for the assessment of left ventricular (LV) dimensions and function, left atrial (LA) dimension, LVOT gradient, and presence of SAM. Standard echocardiographic images were acquired and stored digitally as looped cardiac cycles for later offline analysis. Exercise echocardiography was performed where clinically indicated using treadmill exercise according to a standard Bruce protocol with immediate post-exercise echocardiographic assessment of the LVOT gradient. Follow-up clinical assessment and echocardiography were performed at three months, and six to nine months post-procedure. Cardiac dimensions were measured according to American Society of Echocardiography (ASE) guidelines. Clinical outcomes were analysed by retrospective case note review.
Procedural results
The demographic data of a total of 18 patients considered eligible for ASA are shown in table 1. None of the patients had a family history of sudden cardiac death. Fifteen patients underwent ASA, and in the remaining three cases the procedure was not performed because of unsuitable septal branch anatomy. A mean of 4.75 ml (range 1.5–9.0 ml) of absolute alcohol were injected into the septal perforator artery. Two patients developed transient right bundle branch block (RBBB) and five had transient broadening of the QRS complex, and in all these patients the ECG normalised within 72 hours. Three patients developed complete heart block in the peri-operative period requiring PPM implantation. One patient had a localised dissection of the septal branch of the LAD; the procedure was terminated and a repeat procedure was successful three months later. One patient had a small pericardial effusion, which was managed conservatively. One patient had a right coronary artery stenosis that required percutaneous coronary intervention (PCI); however, breathlessness persisted and the patient then underwent ASA. There was no peri-procedural death. The average duration of in-patient stay was 4.5 ± 2.9 days (range 2–15). Three patients needed PPM implantation due to persistent complete heart block more than five days post-procedure. The average CK level was 1,180 U/L (range 192–2,863 U/L) 12 hours after ablation.
Table 1. Baseline demographic data and symptoms status in total study population (n=18)
Echocardiographic follow-up
There was a significant reduction in ventricular septal thickness within three months of ablation, which continued at six to nine months (table 2). There was also significant improvement in the resting LVOT gradient (figure 3) with a mean at presentation of 98 ± 54 mmHg, improving to 19 ± 17 mmHg within three months of ablation (p<0.001). In 10 out of 15 patients, no resting LVOT gradient was detectable at follow-up. The improvement in LVOT gradient was maintained at six to nine months follow-up (mean gradient 22 ± 21 mmHg, p<0.001 compared with baseline). There was also an observed reduction in SAM and associated mitral regurgitation in 60% of cases. There was no significant change in LV end-diastolic dimension (4.6 ± 0.6 cm vs. 4.5 ± 0.5 cm, p=0.75) or left atrial dimension (4.4 ± 0.6 cm vs. 4.5 ± 0.9 cm, p=0.78) over the course of the study.
Table 2. Echocardiographic measurements at baseline, three months and six to nine months after alcohol septal ablation (n=15)Figure 3. Individual trends in left ventricular outflow tract gradient at baseline, three-month follow-up and sixto- nine month follow-up
Clinical follow-up
Mean duration of follow-up was 36 ± 18 months (range 6–60 months). There was no early (within 30 days) mortality; one patient died three months after the procedure due to a septicaemia secondary to chest infection. During short-term follow-up (three months), 13 out of 15 patients reported significant symptomatic improvement with an associated reduction in the NYHA class as shown in figure 4. Three patients with persistent symptoms at three months follow-up had LVOT gradients of 1, 5 and 27 mmHg, compared with pre-procedure gradients of 100, 50 and 75 mmHg, respectively.
Figure 4. Symptomatic assessment using New York Heart Association (NYHA) classification at baseline (n=15) and more than nine months (n=13) after alcohol septal ablation
The clinical improvement was sustained in the medium term with 10 (67%) patients remaining in NYHA class I–II at nine months. None of the patients had a repeat procedure or required re-admission for cardiac events. Two patients had evidence of paroxysmal atrial fibrillation on ambulatory monitoring post-ablation and eight patients had ambulatory monitoring that did not reveal any arrhythmias. Sixteen patients continued treatment with low-dose beta blocker and one with a calcium antagonist. The three patients who did not undergo ASA were managed conservatively; no patients were referred for surgical myectomy.
Discussion
Patients with HCM associated with symptomatic LVOT obstruction have an impaired quality of life and adverse prognosis.12 Although the presence of LVOT obstruction is an independent predictor of progression to severe heart failure and of death, to date no evidence exists of prognostic benefit associated with the relief of obstruction.
The main finding of our study is that ASA is a well-tolerated and efficacious procedure with few in-hospital complications, even in a relatively elderly group of patients. None of the patients suffered major peri-procedural complications such as in-hospital death, ventricular arrhythmias, cardiac tamponade or distant infarction. Three patients needed permanent pacing, which is consistent with the rates in the published literature.13,14
We also confirm that reduction in septal wall thickness, and consequently LVOT obstruction, continues over the medium term, related to progressive maturation of the ASA-induced scar within the ventricular septum and the associated remodelling of LVOT geometry. The maximum outflow gradient reductions following septal ablation occurred between three and 12 months. Consequently, for those in whom symptoms fail to improve, consideration of a further procedure should be deferred for at least six months. This re-assessment should also include a search for other potential causes of persistent breathlessness, such as diastolic dysfunction, arrhythmias or lung disease. Although none of our patients had a repeat procedure, re-intervention rates in the range of 5% have been reported.15
Concern has previously been raised regarding the potential for an increased rate of scar-related arrhythmia post-ASA13,14 and adverse global left ventricular remodelling. None of our patients had clinical or Holter evidence of ventricular arrhythmias during follow-up. Moreover, there were no significant changes in left ventricular dimensions, suggesting that post-infarct remodelling remains confined to the LVOT. Obstructive HCM may also be associated with progressive left atrial enlargement due to diastolic dysfunction. Left atrial enlargement >46 mm is a marker of disease severity16 and an independent predictor of death in patients undergoing surgical myectomy.17 In our study, the LA dimension did not change significantly and, although the follow-up period was relatively short, the absence of progressive LA dilatation might suggest an improvement in left ventricular diastolic function following relief of obstruction.
According to the ACC/ESC guidelines, septal myectomy should remain the gold-standard treatment, and the use of ASA should be confined to older adults in an attempt to limit the adverse effect of any small increase in the risk of serious arrhythmia. The average age of patients in our study is consistent with this recommendation.
Study limitations
This study consists of a relatively small sample size, reflecting the fact that these data are derived from real-world practice in a highly selected group of patients. Although no major adverse cardiac events were detected during follow-up, assessment of arrhythmias by ambulatory monitoring was not performed on a systematic basis. Therefore, asymptomatic or transient arrhythmias may have been missed, although the exact relevance of this remains unclear.
Conclusions
Our results demonstrate that ASA performed according to current guidelines in a real-world tertiary referral population is a beneficial interventional treatment modality for patients with obstructive HCM refractory to medical treatment. The effect of ASA on long-term prognosis remains to be determined in larger studies with longer follow-up periods.
Conflict of interest
None declared.
Editors’ note
Please see also the editorial by Sekhri et al. on pages 201–02 of this issue.
Key messages
Alcohol septal ablation (ASA) is an alternative therapeutic method in the treatment of symptomatic left ventricular outflow tract (LVOT) obstruction in patients with hypertrophic cardiomyopathy (HCM)
ASA is performed by injecting alcohol into the target septal branch of the left anterior descending coronary artery
Our experience of the technique in a typical sample of patients referred to a tertiary centre confirms that ASA is an effective non-surgical technique for treatment of symptoms related to LVOT obstruction in HCM
Long-term studies of larger populations are necessary to determine the wider prognostic significance of the procedure
References
1. McKenna WJ, Behr ER. Hypertrophic cardiomyopathy: management, risk stratification, and prevention of sudden death. Heart 2002;87:169–76. (doi: 10.1136/heart.87.2.169)
3. Maron BJ, Nishimura RA, McKenna WJ et al. Assessment of permanent dual-chamber pacing as a treatment for drug-refractory symptomatic patients with obstructive hypertrophic cardiomyopathy: a randomized, double-blind, crossover study (M-PATHY). Circulation 1999;99:2927–33.
4. Sigwart U. Non-surgical myocardial reduction for hypertrophic obstructive cardiomyopathy. Lancet 1995;346:211–14. (doi: 10.1016/S0140-6736(95)91267-3)
5. Braunwald E. Induced septal infarction: a new strategy for hypertrophic obstructive cardiomyopathy. Circulation 1997;95:1981–2.
6. Seggewiss H, Gleichmann U, Faber L et al. Percutaneous transluminal septal myocardial ablation in hypertrophic obstructive cardiomyopathy: acute results and 3-month follow-up in 25 patients. J Am Coll Cardiol 1998;31:252–8. (doi: 10.1016/S0735-1097(97)00508-1)
7. Faber L, Meissner A, Ziemsenn P, Seggewiss H. Percutaneous transluminal septal myocardial ablation for hypertrophic obstructive cardiomyopathy: long term follow up of the first series of 25 patients. Heart 2000;83:326–31. (doi: 10.1136/heart.83.3.326)
8. Gietzen FH, Leuner CJ, Raute-Kreinsen U et al. Acute and long-term results after transcoronary ablation of septal hypertrophy (TASH). Catheter interventional treatment for hypertrophic obstructive cardiomyopathy. Eur Heart J 1999;20:1342–54. (doi: 10.1053/euhj.1999.1520)
9. Alam M, Dokainish H, Lakkis NM. Hypertrophic obstructive cardiomyopathy-alcohol septal ablation vs. myectomy: a meta-analysis. Eur Heart J 2009;30:1080–7. (doi: 10.1093/eurheartj/ehp016)
10. Qin JX, Shiota T, Lever HM et al. Outcome of patients with hypertrophic obstructive cardiomyopathy after percutaneous transluminal septal myocardial ablation and septal myectomy surgery. J Am Coll Cardiol 2001;38:1994–2000.
11. Maron BJ, McKenna WJ, Danielson GK et al. American College of Cardiology/European Society of Cardiology Clinical Expert Consensus Document on Hypertrophic Cardiomyopathy a report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents and the European Society of Cardiology Committee for Practice Guidelines. J Am Coll Cardiol 2003;42:1687–713. (doi: 10.1016/S0735-1097(03)00941-0)
12. Maron MS, Olivotto I, Betocchi S et al. Effect of left ventricular outflow tract obstruction on clinical outcome in hypertrophic cardiomyopathy. N Engl J Med 2003;348:295–303. (doi: 10.1056/NEJMoa021332)
13. Alam M, Dokainish H, Lakkis NM. Alcohol septal ablation for hypertrophic obstructive cardiomyopathy: a systematic review of published studies. J Interv Cardio 2006;19:319–27. (doi: 10.1111/j.1540-8183.2006.00153.x)
14. Sorajja P, Nishimura RA, Gersh BJ et al. Outcome of mildly symptomatic or asymptomatic obstructive hypertrophic cardiomyopathy: a long-term follow-up study. J Am Coll Cardiol 2009;54:234–41. (doi: 10.1016/j.jacc.2009.01.079)
15. Kuhn H, Seggewiss H, Gietzen FH et al. Catheter-based therapy for hypertrophic obstructive cardiomyopathy. First in-hospital outcome analysis of the German TASH Registry. Kardiol 2004;93:23–31. (doi: 10.1007/s00392-004-1028-6)
16. Nagueh SF, Lakkis NM, Middleton KJ et al. Changes in left ventricular filling and left atrial function six months after nonsurgical septal reduction therapy for hypertrophic obstructive cardiomyopathy. J Am Coll Cardiol 1999;34:1123–8. (doi: 10.1016/S0735-1097(99)00341-1)
17. Woo A, Williams WG, Choi R et al. Clinical and echocardiographic determinants of long-term survival after surgical myectomy in obstructive hypertrophic cardiomyopathy. Circulation 2005;111:2033–41. (doi: 10.1161/01.CIR.0000162460.36735.71)
In order to determine the taking of regular aspirin within a representative community sample of adults residing in the south Wales county of Caerphilly, we conducted a survey of a sample 9,551 adults resident in the county aged ≥18 years.
Questionnaires were returned by 4,558 individuals aged between 25 and 82 years. Nearly 12% of the respondents reported a previous vascular event. Of these, 68% of the men and 55% of the women stated that they took aspirin regularly. Among those with no previous vascular event, 22% of the men and 13% of the women stated that they took aspirin regularly. For those over 50 years of age, the respective figures were 28% of men and 19% of women. Of those taking aspirin, 47% stated that they took 300 mg tablets. There was a small inverse relationship found between aspirin taking and social class, namely 67% and 56% in the manual and non-manual classes respectively.
The prevalence of prophylactic aspirin taking by persons who have had a vascular event should be increased, particularly in women. Knowledge of the benefits and the risks of aspirin prophylaxis could be promoted through the community and there should be ongoing monitoring of aspirin taking.
Introduction
Daily low-dose aspirin (75–100 mg per day) substantially reduces the risk of subsequent vascular events, such as myocardial infarction and ischaemic stroke.1 Evidence from primary prevention trials has indicated a reduction in the risk of a first vascular event,2 but the benefit–risk balance for this is open to debate.3
The prevalence of aspirin taking by patients at increased vascular risk and by the general population is unknown in the UK. The following reports a survey to determine the taking of regular aspirin within a representative community sample of adult individuals in the south Wales county of Caerphilly.
Methods
The Caerphilly Health and Social Needs Study4 was a postal questionnaire survey of 22,236 individuals randomly sampled from the 132,613 residents aged 18 years and over in May 2001 in the county of Caerphilly. Of the 22,236 questionnaires posted, 12,408 were returned, giving an adjusted response rate of 62.7%, after removal of questionnaires sent to incorrect addresses. A follow-up questionnaire was sent to the 9,551 baseline respondents identified as still living in the county using the NHS Administrative Register in August 2008.
Five questions on aspirin taking were included, with the aim being to ascertain the prevalence of aspirin taking throughout the community and the reasons for taking the medicine or for not taking it. Four questions on the occurrence of prior vascular disease events were assessed to estimate aspirin taking in these groups. The nine specific questions are presented separately in table 1.
Table 1. Questions included in the survey
Results
Questionnaires were returned by 4,798 individuals, giving a response rate of 53%. From these 240 (5%) were removed as their age or sex was different to that recorded in the NHS Administrative Register. The mean age of the other respondents was 56 years and 42.8% were male. Table 2 presents a summary of the prevalence of aspirin taking within the respective age groups and also according to whether or not a previous vascular event had been experienced.
Table 2. The prevalence of aspirin by age, within all individuals and within subjects grouped by whether or not they had had a prior vascular event
Of the respondents, 533 (11.7%, 95% confidence intervals [CI] 10.8%–12.6%) reported a previous vascular event: a heart attack, stroke or deep vein thrombosis. Of these, 62% (95% CI 58%–66%) stated that they were taking aspirin regularly, and just under half (47%) said that they took 300 mg tablets. Almost all (97%) were taking the drug on advice from their doctor. Of the subjects in the Registrar General’s non-manual occupations, 56% (95% CI 49%–63%) were taking aspirin, compared with 67% (95% CI 62%–72%) of the subjects in manual occupations.
A total of 98 (18%) of the 533 subjects who indicated that they had experienced a previous vascular event stated that they could not take aspirin. In free text answers, 43 of these stated that they were taking warfarin, 12 said they were sensitive to aspirin and 22 either experienced gastric irritation from the drug or had a peptic ulcer. Five subjects gave reasons related to bleeding but it was not possible from their responses to judge whether they avoided aspirin because of a fear of bleeding, or had experienced a bleed that had been attributed to aspirin.
The prevalence of aspirin taking in individuals who reported no prior vascular event was 17%. Among the 2,518 respondents aged 50 years or over with no prior vascular event, 28% of the men and 19% of the women (23%, 95% CI 21%–25% combined) said that they took aspirin regularly. Of the subjects in the Registrar General’s non-manual occupations, 21% (95% CI 19%–23%) took aspirin regularly, compared with 26% (95% CI 24%–28%) of those in manual occupations. Of the respondents, 87% stated that they took the drug on their doctors recommendation and just under half (42%) said that they took 300 mg tablets. Among those who rated their general health as ‘good’, 18% (95% CI 16%–20%) took aspirin regularly, while of those who rated themselves as having ‘poor’ health, 35% (95% CI 32%–38%) took it.
Differences in aspirin taking between the social classes were small, but significant. One would not expect a difference among patients who had a previous vascular event, yet 67% of those in manual social classes were taking aspirin, while the prevalence in the non-manual social classes was found to be lower at 56%. A small difference in the same direction was found in the healthy subjects, namely 26% in the manual social classes and 21% in the non-manual.
Discussion
Aspirin is of undoubted benefit in patients who have had a vascular event, and it is concerning, therefore, that the prevalence of aspirin taking in those who had a previous vascular event was 68% (95% CI 63%–73%) in men and significantly lower in women at 55% (95% CI 49%–61%). In a similar survey conducted in 2003 in patients in primary care practices across Wales, a compliance rate of 72% (95% CI 46%–84%) was found in post-infarct patients.5 Given the introduction of the Primary Care Contract in the interval, this lack of improvement is a matter of concern.
These prevalence rates may be compared to those reported from studies in the USA. In one study, the prevalence of aspirin taking by individuals who had had a heart attack or stroke was 83%.6 In those with neither a vascular disease event nor diabetes, aspirin taking was strongly related to the number of vascular risk factors: 21% in those reporting no risk factors to 49% in those reporting four or more factors.6
The inverse relationships with social class, although small, were surprising in that individuals within the manual classes had a higher uptake than non-manual, both for those who had had a vascular event and those who had not. Of the individuals who were taking aspirin, 97% of those with a prior vascular event and 87% of the individuals aged 50 years or over who had not had a vascular event, took the drug on advice from their doctor. However, understanding of the medicine seems to have been limited because around half of the individuals took 300 mg tablets, rather than the low-dose of 70–100 mg usually recommended.
Aspirin prophylaxis has been recommended for all individuals over the age of about 50 years7,8 and the prevalence of aspirin taking by individuals over this age that had not had a prior vascular event was 23%. This appears lower than the estimate of 36% made in a survey in the USA for individuals aged 35–64 years.6
While the treatment of disease is the responsibility of physicians and other healthcare professionals, the preservation of health is ultimately the responsibility of the individual.9 Aspirin is readily available ‘over the counter’ in most countries and one of the responsibilities of those in healthcare is to make the risks and benefits of prophylactic measures, including medicines, clear and readily available. This is to ensure that individuals are equipped to make a well-informed decision. Another factor in this may be the self-evaluation of possible outcomes.
The data we present are limited in that they relate only to a small community within the UK. Clearly, data from a much wider survey would be of value, if evidence from this were complemented with data on hospital admissions attributable to aspirin to assess the undesirable side effects of the medicine. Furthermore, evidence on aspirin taking now may become of increased value and interest if aspirin is promoted for use in screening procedures for colon polyps and for persons with other evidences of an increased cancer risk.10 A key finding of this study is the prevalence of prophylactic aspirin taking by persons who have had a vascular event can be increased, particularly in women. Knowledge of the benefits and the risks of aspirin prophylaxis should be promoted through the community and there should be ongoing monitoring of aspirin taking.
Acknowledgements
The Caerphilly Health and Social Needs Study is funded by the Welsh Assembly Government/MRC Health Research Partnership Award. All the authors read and approved the final manuscript. Peter Elwood and Gareth Morgan were responsible for the questions about aspirin taking and vascular disease and for writing the paper. David Fone, Frank Dunstan and James White carried out the survey, Janet Pickering analysed the data and Clive Mitchell assisted in the interpretation of the results. Michael Martin also assisted in the analysis of the data.
Conflict of interest
None declared.
Key messages
36% of men and 24% of women aged 50 years and over take prophylactic aspirin regularly
Only 68% of men and 55% of women who have had a vascular event take aspirin regularly
Around half of all the individuals on aspirin take 300 mg tablets
There should be better education about low-dose aspirin taking, the risks and benefits and the appropriate dose for prophylaxis
Aspirin taking and hospital admissions attributable to aspirin should be monitored throughout the UK
References
Antithrombotic Trialists’ Collaboration. Collective meta-analysis of randomised trial of antiplatelet therapy for prevention of death, myocardial infarction and stroke in high risk patients. BMJ 2002;324:71–86. (doi:10.1136/bmj.324.7329.71)
Morgan G. Aspirin for primary prevention? Public Health 2009;123:787–8. (doi: 10.1016/j.puhe.2009.10.007)
Antithrombotic Trialists’ Collaboration. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials. Lancet 2009;373:1849–60. (doi: 10.1016/S0140-6736(09)60503-1)
Fone DL, Dunstan FD, Christie S et al. Council tax valuation bands, socio-economic status and health outcome: a cross sectional analysis from the Caerphilly Health and Social Needs Study. BMC Public Health 2006;6:115. (doi: 10.1186/1471-2458-6-115)
Elwood P, Hughes J, Morgan G, Brown G. A survey of aspirin use for vascular prophylaxis in Wales. Quality in Primary Care 2005;119:734–7.
Ajani UA, Ford ES, Greenland KJ. Aspirin use among US adults: Behavioural Risk Factor Surveillance System. Am J Prev Med 2006;30:74–7. (doi: 10.1016/j.amepre.2005.08.042)
Elwood P, Morgan G, Brown G, Pickering J. Aspirin for everyone over 50? BMJ 2005;330:1440–1. (doi: 10.1136/bmj.330.7505.1440)
US Preventive Services Task Force. Aspirin for the prevention of cardiovascular disease: US preventive services task force recommendation statement. Ann Intern Med 2009;150:396–404.
Elwood PC, Longley M. My health – whose responsibility? A jury decides. J Epidemiol Community Health 2010;64:761–4. (doi: 10.1136/jech.2009.087767)
Morgan G, Elwood P. Could aspirin enhance colorectal cancer screening programmes? Eur J Pub Health 2009;19:576–7. (doi: 10.1093/eurpub/ckp062)
Platelet activation is an important part of the pathophysiology of acute coronary syndromes. Inhibition of this by antiplatelet agents forms an important part of the management of this condition. Recently, there has been considerable interest in the variability of platelet response to these drugs and the need to tailor the dose of antiplatelet agents according to the response.
Here, we present a patient who had repeated episodes of stent thrombosis and was found to have decreased response to clopidogrel and aspirin (clopidogrel and aspirin resistance) with the use of the Accumetrics VerifyNowTM analyser. We have also reviewed the literature on this subject.
Our recommendation is that patients who have recurrent stent thrombosis or thrombotic events on dual antiplatelet agents should have their antiplatelet therapy response checked and have their antiplatelet agents tailored accordingly.
Introduction
Activated platelets play a pivotal role in the pathophysiology of acute coronary syndromes, and dual antiplatelet therapy with both aspirin and clopidogrel has become one of the cornerstones of their treatment.1 Similarly, dual antiplatelet therapy is mandated following percutaneous coronary intervention (PCI) with stent insertion to prevent stent thrombosis.2
Recently, there has been considerable interest in the phenomenon of inter-patient variability of clopidogrel response (sometimes termed ‘clopidogrel resistance’)3 and, to a lesser degree, the variability of aspirin response. This has led to interest in tailoring the dose of clopidogrel per patient according to the responsiveness of the platelets to the drug.4 In this report, we describe a patient who suffered recurrent ischaemic coronary events despite dual antiplatelet therapy, and we discuss the various implications of poor antiplatelet response and the current treatment options for similar patients.
Case report
A 41-year-old woman first presented to the rapid access chest pain clinic in May 2007 with a history of exertional angina. Her risk factors were hypertension, hypercholesterolaemia, and a positive family history of ischaemic heart disease (IHD). She had given up smoking three months earlier after a 21 pack-year history. She had a high body mass index of 31 kg/m2 and suffered from hypothyroidism. Exercise electrocardiography (ECG) was positive for symptoms and ECG changes in stage 2 of the Bruce protocol. Subsequent elective coronary angiography demonstrated minor diffuse disease in the left coronary system with a severe ostial right coronary artery (RCA) lesion (figure 1).
Figure 1. Angiographic appearance of ostium of right coronary artery at first presentation
Figure 2. Latest appearance of ostium of right coronary artery showing mild-to-moderate in-stent restenosis
While waiting to undergo elective PCI to her ostial RCA lesion, she was admitted urgently with troponin-positive chest pain and infero-lateral ST-segment shift on an ECG two weeks after her initial presentation. Urgent PCI was performed and a 3 x 16 mm paclitaxel eluting (TaxusTM) stent was placed in the ostium of the RCA. She was discharged on dual antiplatelet therapy.
She presented again a month later, to a local district general hospital with an acute infero-lateral ST-elevation myocardial infarction (STEMI) for which she was treated with thrombolysis. There was no resolution of her ST segments or symptoms and she was transferred to our institution for rescue angioplasty. Angiography at this time revealed a patent RCA stent, but with a thrombotic occlusion of a small posterior left ventricular (PLV) branch. It was likely that she had subacute stent thrombosis, and the thrombolysis had largely dissolved the thrombus, but with a small remnant in the distal vessel. The vessel was wired and a balloon used to disrupt the thrombus. A stent was not deployed as the vessel was of small calibre. She was treated for 24 hours with the glycoprotein IIb/IIIa antagonist, tirofiban, and low molecular weight heparin, and her condition stabilised such that she was subsequently discharged on dual antiplatelet therapy.
She remained fairly well, until 18 months later, when she presented once again to her local hospital with chest pains. ECG on this occasion again showed an inferior STEMI. She was successfully treated with thrombolysis and was transferred for further assessment.
As part of a separate research protocol, platelet function studies were performed using the Accumetrics VerifyNowTM rapid platelet function analyser (RPFA). This showed a raised level of P2Y12 resistance units (PRU) of 363 after 30 days of clopidogrel 75 mg once daily, indicating a poor platelet response to clopidogrel. The same device also demonstrated significant aspirin resistance with aspirin resistance units (ARU) of 630.
Repeat angiography now showed new pressure damping in left main stem (LMS) with mild disease only in the left anterior descending (LAD) and circumflex coronary vessels. There was new late ostial in-stent restenosis (amounting to 50% of the luminal caliber), and a tight ostial PLV lesion (figure 2). A pressure wire study to the LMS was performed and this was positive with a fractional flow reserve (FFRmyo) of 0.77 using adenosine via a central venous catheter. Intravascular ultrasound of the RCA stent revealed that it was well sized and well deployed and the degree of in-stent restenosis confirmed.
In view of the left main stem lesion and recurrent thrombotic episodes, she was referred for coronary artery bypass graft surgery, and following this is taking aspirin alone. She continues to do well following this intervention.
Discussion
There are a number of variables associated with stent thrombosis following PCI, including interventional factors (for example the complexity of the lesion, bifurcating lesions and poor stent expansion and apposition to the vessel wall) and patient variables (such as diabetes mellitus and renal failure).5 Increasingly, it has become clear that poor response to the antiplatelet agents aspirin and/or clopidogrel is associated with ischaemic events post PCI.6,7 A recent study has indicated that the incidence of definite/probable stent thrombosis at six months in patients undergoing PCI with drug-eluting stents and dual antiplatelet therapy resistance (as in our case above) is over 13%.6 Similarly, reduced clopidogrel activity, as measured using Accumetrics VerifyNow RPFA, has recently been shown to be independently predictive of cardiovascular death and nonfatal myocardial infarction 12 months following stent insertion.8
While the gold-standard test of platelet activity, optical platelet aggregometry, has been extensively used to assess the response to clopidogrel and aspirin in research protocols, it is a complex and time-consuming technique, requiring a high degree of expertise. It is unlikely, therefore, to find widespread acceptance as a routine clinical tool. The recent development of simple near-patient platelet function analysers, such as the VerifyNow RPFA, allows rapid and reproducible assessment of platelet response to aspirin and clopidogrel.9 There is also an increasing body of evidence indicating that poor RPFA results might predict clinical outcome, however, as yet, there are no definite guidelines providing a clinical definition of clopidogrel or aspirin resistance. It has been suggested that an aspirin resistance unit (ARU) level >550 indicates clinically important hyporesponsiveness, and this level has been shown to predict post-PCI myonecrosis.10 Two recent papers have identified the clinically relevant cut-off point of clopidogrel resistance to predict subsequent negative clinical events for RPFA PRU as 23511 and 240.12 As the weight of evidence supporting the use of near-patient tests for this purpose increases, interventional cardiologists need to decide whether to apply this technology in their own departments.
An ongoing issue is that if patients are identified as non-responders to clopidogrel, there is no current consensus on how best to manage their risk of recurrent ischaemic events. However, there is increasing evidence that in poor responders, increasing the clopidogrel dose from 75 mg to 150 mg daily improves antiplatelet activity,13,14 and that the increased doses may reduce clinical adverse events.15
This case illustrates the importance of antiplatelet resistance and we suggest that all patients with acute or subacute stent thrombosis should have their stent investigated using intravascular ultrasound to exclude a mechanical cause for the thrombosis. If none is found, platelet function testing using a validated method should be undertaken to exclude significant antiplatelet hyporesponsiveness.
Conflict of interest
None declared.
References
Anderson JL, Adams CD, Antman EM et al. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction) developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. J Am Coll Cardiol 2007;50:e1–e157. (doi: 10.1016/j.jacc.2007.02.013)
King SB, Smith SC, Hirshfeld JW et al. 2007 focused update of the ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines: (2007 Writing Group to Review New Evidence and Update the 2005 ACC/AHA/SCAI Guideline Update for Percutaneous Coronary Intervention). Circulation 2008;117:261–95. (doi: 10.1161/CIRCULATIONAHA.107.188208)
Serebruany VL, Steinhubl SR, Berger PB et al. Variability in platelet responsiveness to clopidogrel among 544 individuals. J Am Coll Cardiol 2005;45:246–51. (doi: 10.1016/j.jacc.2004.09.067)
Bonello L, Camoin-Jau L, Arques S et al. Adjusted clopidogrel loading doses according to vasodilator-stimulated phosphoprotein phosphorylation index decrease rate of major adverse cardiovascular events in patients with clopidogrel resistance: a multicenter randomized prospective study. J Am Coll Cardiol 2008;51:1404–11. (doi: 10.1016/j.jacc.2007.12.044)
Kuchulakanti PK, Chu WW, Torguson R et al. Correlates and long-term outcomes of angiographically proven stent thrombosis with sirolimus- and paclitaxel-eluting stents. Circulation 2006;113:1108–13. (doi: 10.1161/CIRCULATIONAHA.105.600155)
Gori AM, Marcucci R, Migliorini A et al. Incidence and clinical impact of dual nonresponsiveness to aspirin and clopidogrel in patients with drug-eluting stents. J Am Coll Cardiol 2008;52:734–9. (doi: 10.1016/j.jacc.2008.05.032)
Buonamici P, Marcucci R, Migliorini A et al. Impact of platelet reactivity after clopidogrel administration on drug-eluting stent thrombosis. J Am Coll Cardiol 2007;49:2312–17. (doi: 10.1016/j.jacc.2007.01.094)
Marcucci R, Gori AM, Paniccia R et al. Cardiovascular death and nonfatal myocardial infarction in acute coronary syndrome patients receiving coronary stenting are predicted by residual platelet reactivity to ADP detected by a point-of-care assay: a 12-month follow-up. Circulation 2009;119:237–42. (doi: 10.1161/CIRCULATIONAHA.108.812636)
Godino C, Mendolicchio L, Figini F et al. Comparison of VerifyNow-P2Y12 test and Flow Cytometry for monitoring individual platelet response to clopidogrel. What is the cut-off value for identifying patients who are low responders to clopidogrel therapy? Thromb J 2009;7:4. (doi: 10.1186/1477-9560-7-4)
Chen WH, Lee PY, Ng W, Tse HF, Lau CP. Aspirin resistance is associated with a high incidence of myonecrosis after non-urgent percutaneous coronary intervention despite clopidogrel pretreatment. J Am Coll Cardiol 2004;43:1122–6. (doi: 10.1016/j.jacc.2003.12.034)
Price MJ, Endemann S. Prognostic significance of post-clopidogrel platelet reactivity assessed by a point-of-care assay on thrombotic events after drug-eluting stent implantation. Eur Heart J 2008;29:992–1000. (doi: 10.1093/eurheartj/ehn046)
Marcucci R, Gori AM, Paniccia R et al. Cardiovascular death and nonfatal myocardial infarction in acute coronary syndrome patients receiving coronary stenting are predicted by residual platelet reactivity to ADP detected by a point-of-care assay: a 12-month follow-up. Circulation 2009;119:237–42. (doi: 10.1161/CIRCULATIONAHA.108.812636)
Angiolillo DJ, Shoemaker SB, Desai B et al. Randomized comparison of a high clopidogrel maintenance dose in patients with diabetes mellitus and coronary artery disease: results of the Optimizing Antiplatelet Therapy in Diabetes Mellitus (OPTIMUS) study. Circulation 2007;115:708–16. (doi: 10.1161/CIRCULATIONAHA.106.667741)
Aleil B, Jacquemin L, De Poli F et al. Clopidogrel 150 mg/day to overcome low responsiveness in patients undergoing elective percutaneous coronary intervention: results from the VASP-02 (Vasodilator-Stimulated Phosphoprotein-02) randomized study. J Am Coll Cardiol Cardiovasc Interv 2008;1:631–8. (doi: 10.1016/j.jcin.2008.09.004)
Bonello L, Camoin-Jau L, Arques S et al. Adjusted clopidogrel loading doses according to vasodilator-stimulated phosphoprotein phosphorylation index decrease rate of major adverse cardiovascular events in patients with clopidogrel resistance: a multicenter randomized prospective study. J Am Coll Cardiol 2008;51:1404–11. (doi: 10.1016/j.jacc.2007.12.044)
Department of Cardiology, Royal Hospital, Post Box 1331,
Muscat-111, Sultanate of Oman
A 27-year-old Arab woman with history of seronegative rheumatoid arthritis for four years presented with a three-day history of multiple joint pains and swelling, along with fever. Clinically, she had bilateral rheumatoid hand deformities with signs of active arthritis of elbows, hands and knee joints. She was in sinus rhythm with normal cardiac examination. She was treated with steroids and was responding well except for mild fever, for which an echocardiogram was requested to rule out infective endocarditis.
Images from her transthoracic and transoesophageal echocardiogram showed two large (2 cm2) left atrial nodular masses; one attached to the atrial surface of the anterior mitral leaflet tip and another free-floating in the left atrium, but not causing any mitral valve obstruction (figure 1). The mitral leaflets appeared normal with no regurgitation and no masses were noted in other chambers or valves including atrial appendages. A differential diagnosis of vegetations, thrombus or tumour mass was considered. Three sets of blood cultures were negative. A thrombophilia screen demonstrated markedly raised IgG anticardiolipin, β2 glycoprotein I antibodies and a positive lupus anticoagulant. Her anti-nuclear antibody and anti-double-stranded DNA were positive, confirming the diagnosis of systemic lupus erythematosus (SLE). Her anti-cyclic citrullinated peptide was positive, suggesting a diagnosis of ‘rhupus’, an overlap between rheumatoid arthritis and SLE.1
Figure 1. Transthoracic (A, B) and trans-oesophageal (C) echocardiography showing the presence of a large nodular free-floating left atrial thrombus along with a nodular thrombus attached to anterior mitral valve leaflet (arrow heads) in a patient with rhupus and secondary antiphospholipid syndrome
She also had an incidental finding of bilateral external jugular vein thrombosis detected during computed tomography of neck, chest and abdomen. The patient was managed with intravenous heparin followed by high intensity oral warfarin. Her follow-up echocardiograms showed complete resolution of both masses by four weeks without any systemic embolism (figure 2). Her antiphospholipid antibodies along with lupus anticoagulant repeated at three months were positive, confirming secondary antiphospholipid syndrome according to Sapporo criteria.2
Figure 2. Transthoracic echocardiography repeated after four weeks of oral anticoagulation showed complete resolution of intracardiac thrombi in a patient with rhupus and secondary antiphospholipid syndrome
Discussion
Antiphospholipid syndrome (APS) is an autoimmune disease characterised by antiphospholipid (aPL) antibodies and at least one clinical manifestation, the most common being venous or arterial thrombosis and recurrent fetal loss. The syndrome occurs in isolation (primary APS) or in association with connective tissue diseases (secondary APS), particularly SLE.2 Heart valve lesions (vegetations, valve thickening and dysfunction) are frequent in APS, independent of SLE.2
Review of literature suggests that there are two distinct types of vegetations in patients with APS associated with or without systemic emboli. Libman-Sacks vegetations3 described specifically in SLE are sterile fibrofibrinous masses that are typically sessile, wart-like (verrucoid) and small, varying from pinhead size to 3–4 mm. In addition, Roldan et al.4 have noted that thrombotic vegetations occur in lupus patients due to a hypercoagulable state and that these vegetations (also called non-bacterial thrombotic endocarditis) cannot be clearly differentiated from Libman–Sacks vegetations on echocardiography. There are many case reports describing the occurrence of thrombotic vegetations in patients with APS either as single or multiple masses, which usually resolve on anticoagulation therapy.5,6
In our patient, the occurrence of free-floating mass in association with an isolated mitral valve leaflet mass, along with evidence of thrombosis at another site and typical laboratory abnormalities, favoured the diagnosis of intracardiac thrombi in a patient with APS. Free-floating ball thrombi are usually seen in patients with rheumatic mitral stenosis and, to our knowledge, this has never been described in a patient with APS and rhupus. Treatment of thrombotic vegetations in patients with APS without significant valve dysfunction is controversial. Individual case reports5,6 have noted favourable response to anticoagulation, as seen in our patient. In contrast, long-term follow-up studies have reported that anticoagulant and/or antiplatelet therapy are ineffective in terms of valvular lesion regression.7
In conclusion, this case illustrates that intracardiac thrombi may precede other manifestations of APS. It also highlights the need to screen young patients with intracardiac masses of unknown aetiology for aPL antibodies.
Conflict of interest
None declared.
References
Amezcua-Guerra LM, Springall R, Marquez-Velasco R, Gomez-García L, Vargas A, Bojalil R. Presence of antibodies against cyclic citrullinated peptides in patients with ‘rhupus’: a cross-sectional study. Arthritis Res Ther 2006;8:R144. (doi: 10.1186/ar2036)
Miyakis S, Lockshin MD, Atsumi T et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J Thromb Haemost 2006; 4:295–306. (doi: 10.1111/j.1538-7836.2006.01753.x)
Hojnik M, George J, Ziporen L, Shoenfeld Y. Heart valve involvement (Libman–Sacks endocarditis) in the antiphospholipid syndrome. Circulation 1996;93:1579–87.
Roldan CA, Shively BK, Crawford MH. An echocardiographic study of valvular heart disease associated with systemic lupus erythematosus. N Engl J Med 1996;335:1424–30. (doi: 10.1056/NEJM199611073351903)
Agirbasli MA, Hansen DE, Byrd III BF. Resolution of vegetations with anticoagulation after myocardial infarction in primary antiphospholipid syndrome. J Am Soc Echocardiogr 1997;10:877–80. (doi: 10.1016/S0894-7317(97)70050-6)
Salzberg SP, Nemirovsky D, Goldman ME, Adams DH. Aortic valve vegetation without endocarditis. Ann Thorac Surg 2009;88:267–9. (doi: 10.1016/j.athoracsur.2008.10.006)
Turiel M, Sarzi-Puttini P, Peretti R et al. Five-year follow-up by transesophageal echocardiographic studies in primary antiphospholipid syndrome. Am J Cardiol 2005;96:574–9. (doi: 10.1016/j.amjcard.2005.04.022)
Outcome in patients with peripartum cardiomyopathy (PPCM) is variable. Recovery of left ventricular function is observed in between 23% and 51% of cases at six months after diagnosis. Despite standard medical therapy, both morbidity and mortality remain high. Recent evidence has suggested that dopamine-receptor agonists may be beneficial in the treatment of this condition. We describe a case of a patient with PPCM who developed rapid normalisation of left ventricular function following addition of carbergoline, a long-acting dopamine-receptor agonist, to her conventional heart failure therapy.
Case report
A 25-year-old primigravida with a twin pregnancy was admitted with eclampsia at 37 weeks’ gestation following a brief, witnessed, tonic-clonic seizure at home. Prior to admission her pregnancy had been uncomplicated with normal blood pressure (BP) recordings throughout. Her past medical history was unremarkable and there was no family history of cardiomyopathy. On arrival at the emergency department, she was unconscious (Glasgow coma scale [GCS] 7/15) and markedly hypertensive (BP 170/100 mmHg) with 3+ proteinuria on urinalysis. Physical examination revealed normal cardiovascular, respiratory and abdominal systems. Following administration of intravenous magnesium sulphate, her BP improved. She was intubated and ventilated, and emergency caesarean section was performed with delivery of two healthy twin babies. Her BP normalised and she experienced no further seizures. She was extubated on the second day of admission.
On the third day of admission, she experienced dyspnoea, orthopnoea and cough. Physical examination revealed normal BP, sinus tachycardia (110 beats per minute), raised jugular venous pressure, lung crackles on chest auscultation and bilateral pedal oedema. An electrocardiogram (ECG) confirmed sinus tachycardia with no ST-segment changes. Routine blood investigations including full blood count, blood sugar, renal profile and liver function tests were all within normal range. However, her cardiac enzymes were mildly elevated with creatinine kinase 317 U/L (24–173) and troponin T 0.18 ug/L (0–0.10). Chest radiography revealed pulmonary congestion (figure 1).
A transthoracic echocardiogram performed the same day revealed a normal-sized left ventricle (left ventricular end diastolic [LVED] diameter 4.3 cm, left ventricular end systolic [LVES] diameter 3.5 cm) with severe impairment of systolic function (ejection fraction 25%) (figure 2). There was severe hypokinesia of the posterior wall and apical segments. No valvular disease or left ventricular hypertrophy was detected. The patient was treated with an intravenous diuretic (frusemide) and an angiotensin-converting enzyme (ACE) inhibitor (enalapril) with subsequent clinical improvement. A beta blocker (bisoprolol) was added once her condition had stabilised.
Figure 2. A. Transthoracic echocardiogram on the third day postpartum demonstrated severe left ventricular systolic dysfunction with profound hypokinesia of the posterior wall. B. Following carbergoline treatment, repeat transthoracic echocardiography two weeks postpartum revealed dramatic recovery of left ventricular function
Further laboratory investigations included negative viral and auto-antibody screens. Breastfeeding was discouraged in view of her pharmacotherapy and the possibility of mother-to-baby drug transmission. Since the patient was not lactating, she was administered a long-acting dopamine-receptor agonist, oral cabergoline (0.25 mg twice daily for two days), to stop breast milk production and prevent uncomfortable breast engorgement. This treatment was initiated 48 hours after the onset of her cardiac symptoms. The patient remained well during the remainder of her admission. Attempts at increasing her medication as prophylaxis against heart failure resulted in the development of hypotension, and so she was eventually discharged on frusemide 40 mg once daily, enalapril 5 mg once daily and bisoprolol 1.25 mg once daily. A repeat echocardiogram two weeks postpartum revealed that her left ventricular function had normalised (ejection fraction 79%) with complete resolution of the previously documented regional wall motion abnormalities. She remained asymptomatic and continued on the same doses of ACE inhibitor and beta blocker treatment.
Discussion
PPCM is a rare cardiomyopathy that can affect women at any time from the last month of pregnancy up until five months after delivery. Diagnosis requires documentation of poor left ventricular function in the absence of other identifiable causes of heart failure.1 The precise aetiology of PPCM is unknown but there is some evidence to implicate an underlying myocarditis. O’Connell et al. observed that 29% of patients with PPCM had myocarditis confirmed by endomyocardial biopsy, in comparison to only 9% of patients with idiopathic dilated cardiomyopathy (DCM).2 In another study by Midei et al., 14 of 18 patients with PPCM were demonstrated to have histologically proven myocarditis.3 Several triggers for myocyte injury have been postulated including viral infection, autoimmune disease, hormonal changes, genetic disorders or toxaemia.4,5
Our patient developed heart failure three days postpartum, which is in keeping with PPCM. This diagnosis is further supported by echocardiographic demonstration of depressed left ventricular function in the absence of other identifiable causes of heart failure. The patient had established risk factors for the development of PPCM including multiple pregnancy and pre-eclampsia.
We do not believe that severe hypertension was contributory to her heart failure since it was transient and she was normotensive in the period preceding her decompensation. Although neurogenic stunned myocardium is a well-established complication of central nervous system disorders, this clinical entity has most commonly been reported with intractable seizures due to status epilepticus.6,7 It is unlikely that the single, self-limiting seizure in our case would have produced a sufficient catecholamine surge to cause such profound myocardial stunning. Furthermore, presentation of neurogenic stunned myocardium typically mimics acute myocardial infarction and manifests as Takotsubo cardiomyopathy, whereas our patient had no evidence of ECG abnormalities or apical ballooning to corroborate this.
The prognosis of patients with PPCM is difficult to predict, with published rates of left ventricular function recovery varying between 23% and 51%.8,9 With standard medical treatment, improvement in left ventricular function is typically observed to occur after at least six months of diagnosis.10 The mainstay of treatment is similar to other forms of cardiomyopathy, namely ACE inhibitor (or angiotensin-receptor blocker), beta blockers, aldosterone antagonist, diuretics and digoxin.
There have been several encouraging reports regarding the use of bromocriptine, a short-acting dopamine-receptor agonist, in PPCM.11,12 More recently, a proof-of-concept pilot study has shown that addition of bromocriptine to standard heart failure therapy improved left ventricular ejection fraction in a small cohort of women with newly diagnosed PPCM.13 Bromocriptine inhibits the release of prolactin, which is secreted from the anterior pituitary gland during pregnancy and postpartum period and stimulates lactation. Animal experiments have shown that prolactin is cleaved into a 16 kDa form as a result of oxidative stress. The 16 kDa prolactin is both anti-angiogenic and pro-apoptotic and may, therefore, mediate PPCM.14 In keeping with this theory, Hilfiker-Kleiner et al. demonstrated that forced generation of 16 kDa prolactin induces a PPCM phenotype in mice.15 Furthermore, treatment with bromocriptine prevented development of PPCM in this murine model. Inhibition of prolactin secretion may, therefore, constitute a novel therapeutic strategy for women with this condition.
Our patient’s symptoms were initially relieved by standard heart failure treatment consisting of diuretics and ACE inhibition with subsequent addition of a beta blocker. However, the rapid normalisation of the left ventricular function observed within two weeks of PPCM diagnosis has never previously been described on this conventional therapy. The low doses of ACE inhibitor and beta blocker treatment administered would be unlikely to account for the dramatic change in left ventricular function in such a short time interval. We, therefore, suggest that the introduction of cabergoline contributed to the rapid improvement in left ventricular function observed.
Both bromocriptine and cabergoline are ergoline derivatives but, unlike bromocriptine, cabergoline has an extremely long half-life (c. 65 hours) and is highly selective for the dopamine D2-receptor. Although several reports have documented the potential efficacy of bromocriptine in PPCM, to the best of our knowledge there is only one other published case report that describes the use of cabergoline.16 However, in contrast to that report, where only partial left ventricular recovery was observed, cabergoline treatment in our patient was associated with complete normalisation of left ventricular function.
Conclusion
Our case illustrates the potential therapeutic benefit of cabergoline, a dopamine-receptor agonist, as an adjunct to facilitate early recovery of left ventricular function in PPCM. Whether or not this will translate to an improvement in the overall prognosis of patients with PPCM remains to be seen. In view of the rarity of this condition, a collaborative multi-centre research strategy is required to further evaluate the efficacy of carbergoline therapy.
Conflict of interest
AG recieves salary support from CORDA.
References
Pearson GD, Veille JC, Rahimtoola S et al. Peripartum cardiomyopathy: National Heart, Lung, and Blood Institute and Office of Rare Diseases (National Institutes of Health) workshop recommendations and review. JAMA 2000;283:1183–8. (doi: 10.1001/jama.283.9.1183)
O’Connell JB, Costanzo-Nordin MR, Subramaniam R et al. Peripartum cardiomyopathy: clinical, hemodynamic, histologic and prognostic characteristic. J Am Coll Cardiol 1986;8:52–6. (doi: 10.1016/S0735-1097(86)80091-2)
Midei M, DeMent S, Feldman A, Hutchins G, Baughman K. Peripartum myocarditis and cardiomyopathy. Circulation 1990;81:922–8. (doi: 10.1161/01.CIR.81.3.922)
Ntusi NBA, Mayosi BA. Aetiology and risk factors of peripartum cardiomyopathy: a systematic review. Int J Cardiol 2009;131:168–79. (doi: 10.1016/j.ijcard.2008.06.054)
Sanderson JE, Olsen EG, Gatei D. Peripartum heart disease: an endomyocardial biopsy study. Br Heart J 1986;56:285–91. (doi: 10.1136/hrt.56.3.285)
Shimizu M, Kagawa A, Takano T, Masai H, Miwa Y. Neurogenic stunned myocardium associated with status epilepticus and postictal catecholamine surge. Intern Med 2008;47:269–73. (doi: 10.2169/internalmedicine.47.0499)
Lemke DM, Hussain SI, Wolfe TJ et al. Tako-Tsubo cardiomyopathy associated with seizures. Neurocrit Care 2008;9:112–17. (doi: 10.1007/s12028-008-9075-x)
Sliwa K, Foster O, Libhaber E et al. Peripartum cardiomyopathy: inflammatory markers as predictors of outcome in 100 prospectively studied patients. Eur Heart J 2006;27:441–6. (doi: 10.1093/eurheartj/ehi481)
Hu CL, Li YB, Zou YG et al. Troponin T measurement can predict persistent left ventricular dysfunction in peripartum cardiomyopathy. Heart 2007;93:488–90. (doi: 10.1136/hrt.2006.087387)
Sliwa K, Skudicky D, Bergemann A, Candy G, Puren A, Sareli P. Peripartum cardiomyopathy: analysis of clinical outcome, left ventricular function, plasma levels of cytokines and Fas/APO-1. J Am Coll Cardiol 2000;35:701–05. (doi: 10.1016/S0735-1097(99)00624-5)
Hilfiker-Kleiner D, Meyer GP, Schieffer E et al. Recovery from postpartum cardiomyopathy in 2 patients by blocking prolactin release with bromocriptine. J Am Coll Cardiol 2007;50:2354–5. (doi: 10.1016/j.jacc.2007.10.006)
Habedank D, Kuhnle Y, Elgeti T, Dudenhausen JW, Haverkamp W, Dietz R. Recovery from peripartum cardiomyopathy after treatment with bromocriptine. Eur J Heart Fail 2008;10:1149–51. (doi: 10.1016/j.ejheart.2008.09.001)
Sliwa K, Blauwet L, Tibazarwa K et al. Evaluation of bromocriptine in the treatment of acute severe peripartum cardiomyopathy: a proof-of-concept pilot study. Circulation 2010;121:1465–73. (doi: 10.1161/CIRCULATIONAHA.109.901496)
Hilfiker-Kleiner D, Schieffer E, Meyer GP, Podewski E, Drexler H. Postpartum cardiomyopathy. Dtsch Arztebl Int 2008;105:751–6.
Hilfiker-Kleiner D, Kaminski K, Podewski E et al. A cathepsin D-cleaved 16 kDa form of prolactin mediates postpartum cardiomyopathy. Cell 2007;128:589–600. (doi: 10.1016/j.cell.2006.12.036)
De Jong JSSG, Rietveld K, van Lochem LT, Bouma BJ. Rapid left ventricular recovery after cabergoline treatment in a patient with peripartum cardiomyopathy. Eur J Heart Fail 2009;br 11:220–2. (doi: 10.1093/eurjhf/hfn034)
The glucagon-like peptide-1 (GLP-1) receptor agonists are a new class of injected drugs for the treatment of type 2 diabetes. They mimic the action of GLP-1 and increase the incretin effect in patients with type 2 diabetes, stimulating the release of insulin. They have additional effects in reducing glucagon, slowing gastric emptying, and inducing satiety. In clinical practice they are associated with significant reductions in glycosylated haemoglobin (HbA1c), weight loss and a low risk of hypoglycaemia. Beneficial effects have also been observed on blood pressure and lipids. The possibility of cardiovascular benefit is now being formally examined in large randomised-controlled trials with primary cardiovascular end points.
Authors: Susan Connolly, Annie Holden, Elizabeth Turner, Gillian Fiumicelli, Juliet Stevenson, Mandeep Hunjan, Alison Mead, Kornelia Kotseva, Catriona Jennings, Jennifer Jones, David A Wood
Consultant Cardiologist and Honorary Senior Lecturer
Gillian Fiumicelli
Cardiovascular Nurse
Juliet Stevenson
Physical Activity Specialist
Mandeep Hunjan
Dietitian
Alison Mead
Chief Dietitian
Kornelia Kotseva
Honorary Consultant Cardiologist
Catriona Jennings
Research Cardiovascular Nurse
Jennifer Jones
Chief Superintendent Physiotherapist
David A Wood
Garfield Weston Professor of Cardiovascular Medicine
International Centre for Circulatory Health, Imperial College, 59-61
We developed and piloted an innovative family-centred preventive cardiology programme (MyAction) that aimed to both integrate the care of patients with vascular disease with that of individuals identified at high multi-factorial risk and help them achieve recommended lifestyle, medical risk factors and therapeutic targets. The 16-week nurse-led programme was delivered by a multi-disciplinary team, including a dietitian, physical activity specialist and cardiologist, in a community setting. Of 206 patients who attended the initial assessment, 54% attended with their partner and 142 patients completed the programme (69%). By the end of the programme, there was a significant improvement seen in adherence to a Mediterranean diet, as well as substantial increases in physical activity levels supported by objective evidence of improved functional capacity. These changes contributed to significant reductions in body mass index (BMI), weight and abdominal obesity. Very similar changes were seen in partners. Blood pressure control also improved significantly, as did achievement of the low-density lipoprotein (LDL)-cholesterol target, and there was a significant increase in the use of cardioprotective medication. Quality of life also improved in both patients and partners. The significant changes achieved by the MyAction preventive cardiology programme should substantially reduce the cardiovascular risk of these patients and their partners in the future.
Introduction
The Founder MyAction team. Front row, from left: Annie Holden, Alison Mead. Back row, from left: Sarah McMeckan, Juliet Stevenson, Catriona Jennings and Gillian Fiumicelli
The Government white paper put ‘prevention first’ because there is strong evidence that a healthy lifestyle, control of other risk factors and cardioprotective medications can substantially reduce cardiovascular disease (CVD).1
Patient priorities for prevention are defined in the Joint British Societies’ Guidelines (JBS2): established vascular disease; asymptomatic high total risk of developing CVD (JBS2 CVD risk ≥20%); and these guidelines, together with the British Association for Cardiac Rehabilitation (BACR) standards, have defined quality care.2,3 Yet, preventive care for these patients is less than optimal.4
The National Audit of Cardiac Rehabilitation shows that only 38% of eligible coronary patients accessed rehabilitation programmes in 2009,5 and patients with exertional angina, the most common presentation of coronary artery disease,6 are not usually included, and nor are other patients with atherosclerotic disease. The new NHS Health Checks programme will result in many more individuals being identified at high multifactorial risk,1 so there is a pressing need for an effective, evidence-based preventive cardiology model for secondary and primary prevention.
We undertook the EUROACTION study, a cluster randomised-controlled trial of a preventive cardiology programme in hospital and primary care, across eight countries in Europe.7 One-year outcomes showed that a nurse-managed, multi-disciplinary, family approach, yielded significant lifestyle improvements and risk factor reductions for both coronary patients (COR), high-risk individuals (HRI) and partners (PR), compared with usual care.8
We developed the MyAction model for the National Health Service (NHS) by integrating the care of those with coronary disease with that of HRI in a community setting, all based on the principles of EUROACTION. The pilot programme was led by a cardiac specialist nurse (nurse prescriber), and the multi-disciplinary team (MDT) included a dietitian, a physical activity specialist and a visiting cardiologist. We set up the first MyAction programme in a public leisure centre in Bromley in partnership with Mytime Active, a leisure trust, and the primary care trust (PCT). This paper describes end of programme results.
Methods
COR were recruited from the Princess Royal Hospital: acute myocardial ischaemia (troponin negative) and stable angina (not eligible for the hospital cardiac rehabilitation programme). HRI were referred from local general practices.
We developed a health professional manual (HPM) for lifestyle and risk factor assessment and management. At initial assessment (IA), patients and partners were seen as couples, but individually assessed by each MDT member for: smoking habit (breath CO); diet (diet history, food habit questionnaire and Mediterranean diet score9); weight and height, body mass index (BMI) and waist circumference; physical activity levels (seven-day physical activity recall) and functional capacity (Chester step test10); psychosocial measures (Dartmouth CO-OP, EuroQol EQVAS and Hospital Anxiety and Depression Scale [HADS]); blood pressure (BP), fasting lipids and glucose; and use of cardioprotective medications. This assessment identified the couple’s priorities and needs to reduce their cardiovascular risk, as well as exploring beliefs, barriers and motivators to change. Motivational interviewing and goal setting were used. The 16-week programme included individualised follow-up, a weekly educational workshop and supervised exercise session in which all members of the MDT took part. A weekly meeting between the MDT and cardiologist reviewed lifestyle, risk factor and therapeutic goals, and the nurse and cardiologist followed protocols (HPM) for risk factor management including medication as appropriate (figure 1).
Figure 1. Overview of the MyAction programme
After programme completion, the couple had an end of programme (EOP) assessment, which recorded the same data as at IA. Data were stored on a secure electronic database. The outcome measures reported are changes in proportions, between IA and EOP assessment, achieving lifestyle, risk factor and therapeutic targets.3
Statistical analysis
Variables are summarised at IA and EOP using means and standard deviations (SDs) for quantitative measurements, and percentages for binary variables are used. The t-test (or Mann-Whitney test) is used for quantitative measurements to compare those who attended EOP with those who did not. The chi-square test (or Fisher’s exact test) is used for comparison of proportions.
Comparisons of those who had both IA and EOP measurements were made using the paired t-test, Wilcoxon signed-rank test for nonsymmetric distributions and McNemar’s test for paired proportions. Confidence intervals (CIs) for differences in means or proportions were calculated. All significance tests were performed at the 5% level with no adjustment for multiple testing.
Results
Referrals
There were 306 patients (142 COR and 164 HRI) referred to the programme, all of whom were invited to attend an IA. Of these 87 (61%) of COR and 119 (73%) HRI attended: 93 partners (PR) (54% of those with a partner) also attended.
Assessments
Baseline characteristics of patients and partners at IA are shown in table 1. Twenty-two per cent of partners already had a history of either CVD or diabetes mellitus, and a further 21% were subsequently found to have a CVD risk score ≥20% at their initial assessment. Of those who attended IA, 70% (and 63% of partners) attended for an EOP assessment. Those who did not return at EOP were significantly younger (HRI) and more obese (COR) compared with EOP attendees.
Table 1. Baseline characteristics of those who attended the initial assessment
Lifestyle
At IA, 20 patients were current smokers, of whom five (25%) had stopped by EOP (self-reported and CO <6 ppm). Table 2 shows changes between initial and EOP assessment for COR, HRI and PR. Adherence to the Mediterranean diet significantly improved in all three groups. In those overweight at baseline (BMI ≥25 kg/m2), there were significant reductions in mean weight in all three groups, and significant reductions in abdominal obesity in HRI and PRs. At IA, only one fifth of patients and partners were achieving the physical activity target of 30 minutes of moderate intensity aerobic activity five or more times a week, but by EOP, the proportions achieving this target had increased substantially in all three groups. There was also evidence of improved cardiorespiratory fitness with a significant increase in seconds achieved (between 70 and 77 seconds) in the Chester step test in all groups.
Health-related quality of life (HRQoL), as measured by the EQ-VAS and the total Dartmouth CO-OP score, both significantly improved in each patient group and EQVAS alone improved in partners. Significant reductions were also seen in anxiety scores in COR, and in depression scores for both COR and HRI.
Table 2. Lifestyle and anthropometric changes between initial and end of programme (EOP) assessment
Table 3 shows the results for medical risk factors and cardioprotective drugs. There was a significant increase in proportions achieving the BP target in all three groups. There were also significant increases in proportions achieving the total and low-density lipoprotein (LDL)-cholesterol targets; the latter was statistically significant in all three groups. A fasting blood glucose (FBG) was measured in all patients and partners at IA (target ≤6 mmol/L) and glycosylated haemoglobin (HbA1c) was measured in those with known diabetes or newly diagnosed diabetes (FBG >7 mmol/L on two occasions). Only one COR and one HRI were diagnosed with new diabetes at IA. For cardioprotective medication, there was a significant increase in prescription of angiotensin-converting enzyme (ACE) inhibitor/angiotensin-receptor blockers (ARBs) in COR patients; and, in HRI, significant increases in antiplatelet therapy, statins, ACE inhibitors/ARBs and calcium channel blockers occurred.
Table 3. Changes in medical risk factors and prescription of cardioprotective drugs between initial and EOP assessment
Discussion
The MyAction programme offers an innovative approach to secondary and primary prevention in the community. It successfully recruited and retained the majority of patients referred, together with their partners. There was a significant improvement seen in adherence to a Mediterranean diet, as well as substantial increases in physical activity levels supported by objective evidence of improved functional capacity. These changes contributed to significant reductions in BMI, weight and abdominal obesity.
BP control also improved significantly as did achievement of the LDL-cholesterol target. The use of medication in COR was high at IA, but there was also a significant increase in the use of ACE inhibitors/ARBs in both COR and HRI, and statins and calcium channel blockers in HRI alone. Interestingly, although there was no significant increase in medication use in partners, this group also had significant reductions in BP and cholesterol levels, possibly consequent on healthier lifestyle changes. Quality of life also improved in both patients and partners.
The scientific evidence from randomised controlled trials for cardiac rehabilitation and secondary prevention programmes is compelling.11,12 However, in the UK only about a third of coronary patients are accessing such a programme.5 Furthermore, restricting programmes to those who have had surgery or myocardial infarction misses the majority of coronary patients, as the most common presentation is with angina. Moreover, only a minority of cardiac rehabilitation programmes meet the BACR standards in terms of a dedicated MDT, and few provide a comprehensive approach to cardiovascular prevention, the main emphasis being on exercise and physical activity.13 Patients with other forms of atherosclerosis such as transient ischaemic attack (TIA) or peripheral arterial disease, rarely access such programmes, despite having the same disease.
In contrast, the MyAction programme is open to all patients with any presentation of coronary artery disease, or other atherosclerotic disease, and importantly MyAction meets the BACR standards in terms of staffing and also provides all the core components.2
The new NHS Health Checks programme in England will identify those at high total risk of developing CVD.1 Many PCTs are using health trainers to deliver a brief lifestyle intervention and signpost patients to existing local services, including smoking cessation, weight loss programmes and exercise referral schemes. However, there is no evidence that either health trainers or signposting will improve lifestyle and risk factor outcomes.14 In contrast, the MyAction programme provides comprehensive preventive care under one roof for all high-risk patients. Although the meta-analysis of randomised-controlled trials of multi-factorial programmes in primary prevention found no significant effect on total or coronary mortality, a small and potentially important 10% reduction in coronary heart disease (CHD) mortality may have been missed,15 and this apparent lack of effect reflects a modest reduction in smoking and small changes in BP and lipids, the latter due to limited drug treatment in these trials. In contrast, single risk factor trials using drug therapies to lower BP or lipids have shown comparable reductions in CVD risk as predicted by epidemiological relationships.16,17 This pilot of the MyAction programme, like the EUROACTION trial, achieved healthy lifestyle changes, but also significant improvements in the therapeutic control of BP and lipids commensurate with those achieved in the single risk factor trials.
Thus, it is reasonable to postulate that MyAction will substantially reduce total cardiovascular risk in coronary and high-risk patients and their families.
The inclusion of family is important as risk factors for heart disease cluster in families due to shared lifestyles, and there is good evidence that healthy lifestyle change is more likely to occur if the family changes together.18,19 This is supported by the results for partners in the MyAction programme which matched, for the most part, those of the patients.
Study limitations
This is a descriptive study with no control group and, therefore, the results may be due to regression to the mean, not necessarily the effect of MyAction. In addition, not all those who attended IA came back for the EOP assessment, and they had some different characteristics, which is a potential source of bias. However, the statistical analyses presented are based only on those individuals who attended both IA and EOP assessment. Another limitation is the patient population, which was principally white British and from a relatively affluent area in Southeast London. So the MyAction model needs to be validated in different ethnic groups and across all socio-economic strata. This is now taking place in four programmes in NHS Westminster. The lifestyle and risk factor changes described occurred over a short time period (about four months), and it is recognised that such changes may be difficult to maintain over the longer term, although in the EUROACTION trial the same benefits were still evident at one year.8
A MyAction programme is now also being initiated by NHS Heart of Birmingham and more are planned for other parts of the UK. With Westminister, these other programmes will form part of a national demonstration project, which aims to model the cost-effectiveness of the MyAction lifestyle and risk factor outcomes at one year. This will contribute to ongoing evaluation of what is best value for money for prevention in the NHS.
Acknowledgements
We would like to thank. Mike Galvin (Referral Co-ordinator), Dr Ed Langford (Consultant Cardiologist, Princess Royal Hospital, Farnborough), Dr Nada Lemic (Director of Public Health, Bromley PCT), Michaela Nuttall (CHD Coordinator, Bromley PCT), Mr Steve Price (CEO Mytime Active), Angie Sutcliffe (Acute Coronary Syndrome Nurse, Princess Royal Hospital), Clare Schaar (Rapid Access Medical Clinic Nurse, Princess Royal Hospital), Dr Ray Vella (GP CHD Lead, Bromley PCT), and all the general practitioners in Bromley PCT who referred the patients with their families to the programme.
Conflict of interest
The MyAction pilot was funded by an unrestricted educational grant from AstraZeneca UK. SC has received speaker’s honoraria from Merck, Pfizer, AstraZeneca and Abbott Healthcare. AH, ET, GF, JS, MH, AM, KK, CJ, JJ, DAW: none declared.
Key messages
The MyAction preventive cardiology programme is designed to integrate the care of patients with vascular disease with individuals at high multi-factorial risk (JBS2 ≥20%) in a community setting
The 16-week programme is family-centred and delivered by a nurse-led multi-disciplinary team. The foundation of the programme is healthy lifestyle change, management of medical risk factors and prescription of appropriate cardioprotective medication
The results from this pilot in Bromley suggest that the programme was successful in recruiting and retaining the majority of the patients referred, as well as their families, with significant changes achieved in terms of lifestyle, medical risk factors and use of appropriate medication
References
Department of Health. Putting prevention first. Vascular checks: risk assessment and management. London: DoH, 2008.
British Association for Cardiac Rehabilitation. Standards and core components for cardiac rehabilitation. London: BACR, 2007.
Joint British Societies. JBS2: Joint British Societies’ guidelines on prevention of cardiovascular disease in clinical practice. Heart 2009;91(suppl V).
Kotseva K, Wood D, De BG, De BD, Pyorala K, Keil U. EUROASPIRE III: a survey on the lifestyle, risk factors and use of cardioprotective drug therapies in coronary patients from 22 European countries. Eur J Cardiovasc Prev Rehabil 2009;16:121–37.
Sutcliffe SJ, Fox KF, Wood DA et al. Incidence of coronary heart disease in a health authority in London: review of a community register. BMJ 2003;326:20.
Wood DA. EUROACTION: A European Society of Cardiology demonstration project in preventive cardiology. Kotseva K, Jennings C, Mead A et al., editors. A cluster randomized controlled trial of a multi-disciplinary preventive cardiology programme for coronary patients, asymptomatic high risk individuals and their families. Summary of design, methodology and outcomes. Eur Heart J 2005;6(suppl J):J3–J15.
Wood DA, Kotseva K, Connolly S et al. Nurse-coordinated multidisciplinary, family-based cardiovascular disease prevention programme (EUROACTION) for patients with coronary heart disease and asymptomatic individuals at high risk of cardiovascular disease: a paired, cluster-randomised controlled trial. Lancet 2008;371:1999–2012.
Estruch R, Martinez-Gonzalez MA, Corella D et al. Effects of a Mediterranean-style diet on cardiovascular risk factors: a randomized trial. Ann Intern Med 2006;145:1–11.
Sykes K. Chester step test; resource pack(Version 3). Cheshire, UK: Chester College of Higher Education, 1998.
Clark AM, Hartling L, Vandermeer B, McAlister FA. Meta-analysis: secondary prevention programs for patients with coronary artery disease. Ann Intern Med 2005;143:659–72.
Taylor RS, Brown A, Ebrahim S et al. Exercise-based rehabilitation for patients with coronary heart disease: systematic review and meta-analysis of randomized controlled trials. Am J Med 2004;116:682–92.
Brodie D, Bethell H, Breen S. Cardiac rehabilitation in England: a detailed national survey. Eur J Cardiovasc Prev Rehabil 2006;13:122–8.
Kinmonth AL, Wareham NJ, Hardeman W et al. Efficacy of a theory-based behavioural intervention to increase physical activity in an at-risk group in primary care (ProActive UK): a randomised trial. Lancet 2008;371:41–8.
Ebrahim S, Beswick A, Burke M, Davey SG. Multiple risk factor interventions for primary prevention of coronary heart disease. Cochrane Database Syst Rev 2006;(4):CD001561.
Baigent C, Keech A, Kearney PM et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet 2005;366:1267–78.
Law MR, Morris JK, Wald NJ. Use of blood pressure lowering drugs in the prevention of cardiovascular disease: meta-analysis of 147 randomised trials in the context of expectations from prospective epidemiological studies. BMJ 2009;338:b1665.
Pyke SD, Wood DA, Kinmonth AL, Thompson SG. Change in coronary risk and coronary risk factor levels in couples following lifestyle intervention. The British Family Heart Study. Arch Fam Med 1997;6:354–60.
Wood DA, Roberts TL, Campbell M. Women married to men with myocardial infarction are at increased risk of coronary heart disease. J Cardiovasc Risk 1997;4:7–11.
Alan Begg
General Practitioner and Honorary Senior Lecturer Townhead Practice, Montrose, DD10 8TY
Kathryn Griffith
General Practitioner and Clinical CHD Lead Dr Price and Partners, University Health Centre, York University, Heslington, York, YO10 3NP
Reducing morbidity and mortality among post-myocardial infarction (MI) patients requires the implementation of effective secondary measures. This survey examined current practice by assessing the view on, and adherence to, National Institute for Health and Clinical Excellence (NICE) guidance on MI secondary prevention in a sample of general practitioners (GPs) and cardiologists. There were 303 respondents from Scotland and England, including at least 10 GPs and one cardiologist from each English Strategic Health Authority. Although drug treatment post-MI generally complied with NICE recommendations, diet and lifestyle aspects were not implemented fully. There appeared to be sub-optimal integration between primary and secondary healthcare providers. Both GPs and cardiologists underestimated the importance of tailoring secondary prevention services to the individual and the role of omega-3 fatty acid treatments (where required) to supplement dietary intake. There is a clear need to improve compliance of healthcare professionals with many of the key priorities for implementation outlined in the NICE guidelines. In addition, patient-centred cardiac rehabilitation services should be standardised and include strategies to improve patient uptake.
Introduction
Myocardial infarction (MI) is a common condition, estimated to affect almost 150,000 people per year in the UK.1 Without effective treatment, the immediate mortality of MI approaches 40% with a further 10% of patients dying in the subsequent year.2 In those who survive the initial post-MI period, an increased risk of death from cardiovascular causes (5% per year) persists indefinitely.2 However, effective secondary prevention measures can significantly reduce this risk.3
An estimated 1.4 million people in the UK have had an MI.4 Reducing morbidity and mortality among this group requires effective secondary prevention measures. In 2007, the National Institute for Health and Clinical Excellence (NICE) published guidelines on a range of secondary prevention interventions proven to improve outcomes after MI.5 NICE identified the key priorities as: regular physical activity; smoking cessation; Mediterranean-style diet, including two tofour portions of oily fish a week (or omega-3 fatty acid supplementation if appropriate); weight loss where indicated; optimisation of drug treatment; and coronary revascularisation where indicated.5
NICE guidelines recommend delivery of these lifestyle changes through cardiac rehabilitation programmes that are accessible and relevant to all post-MI patients.5 However, implementation of such programmes is inconsistent despite the evidence that rehabilitation reduces cardiac mortality by
27% and has other significant morbidity and quality-of-life benefits.3 The National Audit of
Cardiac Rehabilitation (NACR) estimates that only approximately one-third of post-MI patients enter these programmes, partly due to the variable provision of services across the UK.6 Patient groups, such as women, older patients and ethnic minorities, are underrepresented,7 suggesting that specific patient preferences and requirements are unmet.
Drug therapy for post-MI patients is included in the Quality and Outcomes Framework (QOF) for primary care, and broadly follows the NICE guidance.8 However, limited information is available on the specific implementation of lifestyle recommendations. Thus, the survey reported here explored the care of post-MI patients in England and Scotland, focusing particularly on the specific lifestyle and dietary support, including the prescription of omega-3 fatty acid supplements, offered by general practitioners (GPs) and specialist cardiologists.
Materials and methods
The survey was designed to help understand current patterns of care, highlight opportunities for improving the management of post-MI patients and improve medical education initiatives. A comprehensive series of questions covered all aspects of secondary prevention post-MI. Respondents’ demographic data were also collected. The survey used a combination of dichotomous, multiple-choice and Likert scale formats plus free-text comments, and was conducted within the code of conduct of the Market Research Society and the British Healthcare Intelligence Association. An independent steering committee validated the survey.
Respondents were recruited by Doctors.net.uk, the UK’s largest independent network of primaryand secondary-care physicians. An initial pilot survey with seven respondents (five GPs and two cardiologists) identified any potential ambiguities in the questionnaire. The final survey was released and hosted by Doctors.net.uk during July and August 2009. Survey results were independently analysed.
Respondents were recruited by speciality and geographical location to ensure a sample size of at least 250 GPs and 50 secondary-care specialists/specialist cardiologists representing Scotland and each of the 10 English Strategic Health Authorities. To be eligible to participate, respondents needed to be a GP Principal or Salaried GP, or a cardiologist at Specialist Registrar grade or above (with at least three years’ experience). Respondents received a small honorarium for taking part in the survey.
Results
Respondent demographics
There were a total of 303 respondents (table 1). The majority of GP respondents qualified before 2000, and averaged 1,640 patients on their personal lists. Most of the cardiology specialists were at consultant level or were Specialist Registrars with at least five years’ experience.
Table 1. Demographics of respondents
General aspects of secondary prevention post-MI
Overall, 81% of GP respondents used the NICE guidelines or Scottish Intercollegiate Guidelines Network (SIGN) guidelines to obtain current information on the appropriate care and rehabilitation of post-MI patients. Most cardiologists (>90%) favoured medical journals or conferences for current information but 74% also used the NICE or SIGN guidelines.
Approximately 90% of respondents used regular consultations or involved other healthcare professionals (HCPs) to motivate post-MI patients to pursue a healthy lifestyle. These consultations were most commonly scheduled monthly. However, there was a perception that patient reluctance to engage with HCPs, together with a lack of support from family and friends, were important barriers to the success of lifestyle interventions.
In terms of tailoring secondary prevention programmes to the individual, gender had a minimal influence (mean scores 2.0–2.7 on a scale of 1 [no influence] to 5 [strongly influenced]). By contrast, age was thought more important, particularly when considering exercise (mean score 3.6). Ethnicity was perceived as having little influence on secondary prevention; however, respondents were more likely to take ethnicity into account when delivering dietary advice (mean score 3.1), addressing health and social needs (mean score 2.7–3.0), and tailoring advice to health beliefs or culture (mean score 3.2–3.5).
Dietary and weight loss advice
Of the 13 aspects of post-MI secondary prevention, respondents ranked diet as
fifth in importance after smoking cessation, medication, weight management and exercise (figure 1). There was considerable discrepancy among respondents regarding the primary responsibility for providing dietary advice in the immediate post-MI period. Although ‘dietitian’ was the most frequent response (figure 2), over half of GPs and one-third of cardiologists referred fewer than 20% of their patients to a dietitian. The most common reasons for non-referral were: patient reluctance; long waiting lists; and a perception that patients can make dietary changes without assistance.
Figure 1. Perceived importance of aspects of secondary prevention post-myocardial infarction (MI)Figure 2. Perceived primary responsibility for providing post-MI dietary advice
In total, 98% of respondents personally provided their patients with dietary advice that broadly adhered to NICE guidance. Specifically, more than 80% of respondents advised patients to: reduce consumption of dairy products and replace with unsaturated fats; eat a Mediterranean-style diet containing more bread, fruit and vegetables; increase consumption of oily fish; decrease consumption of salt; and restrict weekly alcohol consumption. Fewer respondents (approximately 50%) advised patients to reduce meat consumption. Less than half felt that their dietary advice was successfully adopted, but only 11% used a food diary to assess patient dietary changes objectively; the majority relied on subjective patient feedback or on indirect measures such as body mass index (BMI) or cholesterol and lipid levels
Despite ranking weight management as the fourth most important component of secondary prevention post-MI, the majority (55%) of respondents provided weight loss counselling to fewer than 60% of obese patients. However, more than 90% advised their patients to take up some form of physical activity.
Smoking cessation
Smoking cessation was considered the most important aspect of secondary prevention. Overall, 99% of respondents assisted with smoking cessation, which correlates with the perceived importance of smoking cessation post-MI. The most common support methods were advice and encouragement, nicotine replacement therapy, and referral to an intensive support service, all of which were used by more than two-thirds of respondents.
Drug therapy
The majority of respondents followed the recommended drug treatment for most post-MI patients (angiotensin-converting enzyme [ACE] inhibitor, aspirin, beta blocker and statin). For patients with left ventricular systolic dysfunction and heart failure, cardiologists were more likely than GPs to prescribe aldosterone antagonists (e.g. eplerenone), in accordance with NICE guidelines. More than half of the cardiologists prescribed aldosterone antagonists for the majority of such patients, compared with just 16% of GPs. Similarly, for patients with ST or non-ST-segment-elevation acute coronary syndrome, cardiologists were more likely than GPs to prescribe clopidogrel in combination with low-dose aspirin.
Despite NICE guidance that omega-3 fatty acid treatment should be considered for patients within three months of an MI who are not achieving the recommended dietary intake of omega-3 fatty acids, more than half of all respondents never prescribed such treatments. Only 11% prescribed them to all or nearly all eligible patients. The primary reason for not prescribing this treatment was adherence to local prescribing recommendations, which do not support use of this treatment despite NICE guidance. However, the perception that patients can consume sufficient omega-3 fatty acids in their diet or can buy products of an adequate strength over-the-counter also contributed. In addition, among doctors who did not prescribe omega-3 fatty acid treatment, there was only mediocre awareness of the clinical benefit (mean score 2.6).
Discussion
The results of this survey indicate that the majority of GPs and cardiology specialists endeavour to follow NICE guidance regarding secondary prevention post-MI. However, these results may be biased towards motivated clinicians with an interest in cardiovascular medicine and may overestimate the application of the NICE guidelines in everyday practice. Furthermore, significant aspects of the NICE guidelines are not being implemented effectively, particularly those relating to diet and lifestyle changes. This may be due to a lack of consistent service provision and confusion over responsibility for initiating rehabilitation measures, suggesting an inadequate integration between primary and secondary healthcare. Similarly, the NACR audit,6 found that a major factor in the poor uptake of cardiac rehabilitation was the failure to deliver a robust patient pathway. This failure is unsurprising as none of the UK cardiac rehabilitation programmes audited by NACR are staffed at the professional level recommended in SIGN guideline 57.9
Our survey also suggests that there is underestimation of the importance of tailoring secondary prevention to the individual – a ‘menu-based’ approach – which may further impact on the uptake and success of rehabilitation programmes. Patients have hugely variable expectations about rehabilitation, and differing motivations for engaging in the services. Health status can also influence uptake of rehabilitation programmes: depression and anxiety are predictors of programme non-attendance.10 Management of these conditions and better support for affected patients within the programmes may improve uptake in some cases. Although not a key point in the NICE guidance, the survey responders perceived management of stress, anxiety and depression as important aspects of secondary prevention (each scoring ≥6.6 out of 10). Patients, therefore, need a comprehensive rehabilitation programme that is appropriate for their individual needs and circumstances. A lack of customisation could be responsible for the reported under-representation of certain patient groups (e.g. women and ethnic minorities) in current rehabilitation programmes.6,7
The importance of dietary change in secondary prevention is particularly under-promoted, despite being a priority in the NICE guidelines. This may arise primarily from confusion over responsibility for providing and assessing dietary advice. Dietitians are underfunded despite evidence of their greater success at effecting dietary change than doctors or other HCPs.11,12 Indeed, NACR reports that 34% of UK cardiac rehabilitation programmes have no dietetic input at all,6 a situation that is likely to worsen in future, with healthcare funding cuts. A perception that dietary advice is not effective in post-MI secondary prevention may also demotivate doctors.
Consistent with the findings of the Myocardial Ischaemia National Audit Project (MINAP),8 this survey demonstrates generally high compliance with NICE guidance on drug therapy for secondary prevention post-MI. In more complex clinical scenarios, cardiologists adhere better to the guidelines than GPs. However, both GPs and cardiologists underrecognise the role of omega-3 fatty acid dietary supplementation. Cost containment through local prescribing restrictions should be resisted to maximise the proven long-term benefits and cost-effectiveness of omega-3 fatty acid treatments in the secondary prevention of MI.13,14 The erroneous belief that dietary intake of omega-3 fatty acids is sufficient, or that over-the-counter formulations are of adequate strength, may also contribute to their lack of use. In reality, patients rarely consume the recommended two-to-four portions of oily fish every week, and over-the-counter preparations typically contain only one-third of the dose of prescription products.15
The cost implications of the NICE guidelines for secondary prevention post-MI are considerable,16 but compelling evidence supports these recommendations3 and they should not be ignored. There is a real and urgent need to comply with key priorities for implementation. Recommended approaches to increase compliance include: improve and standardise provision of patient-centred cardiac rehabilitation services (which may require further development of rehabilitation programmes and increasing staff numbers), use of strategies to improve uptake of these services by patients, and improve adherence by HCPs to the guidelines (table 2).
Table 2. Recommendations to improve secondary prevention post-myocardial infarction (MI) in the UK
Conclusion
In contrast to other chronic disease management initiatives, which are actively promoted and significantly funded, the potential of dietary and lifestyle interventions to reduce morbidity and mortality in post-MI patients is undervalued despite its huge evidence base. It is imperative to improve compliance with the key priorities for implementation outlined in the NICE guidelines, particularly those relating to dietary and lifestyle changes.
Acknowledgement
This survey was funded via an educational grant from Solvay Healthcare.
Conflict of interest
Pope Woodhead and Associates Ltd recruited the Steering Committee, developed the survey and retained full editorial control of the content, including questionnaire development and data analysis. The Steering Committee validated the questionnaire and developed the recommendations arising from the results. Doctors.net.uk hosted the questionnaire and was responsible for independent recruitment. Solvay Healthcare has not had any editorial input into the survey and the opinions expressed in this publication are not necessarily those of Solvay Healthcare. JH, SL, AB, KG, AM, BB: none declared.
Key messages
Significant aspects of the National Institute for Health and Clinical Excellence (NICE) guidelines for secondary prevention post-MI are not being implemented effectively
Only a minority of GPs and cardiologists prescribe omega-3 fatty acid supplements to eligible patients
While rehabilitation services focus on patient-centred strategies to improve uptake and success, only one-third of post-MI patients currently take part in cardiac rehabilitation programmes
Better integration between primary and secondary healthcare throughout the UK could improve the provision of a consistent, standardised cardiac rehabilitation service
Law MR, Watt HC, Wald NJ. The underlying risk of death after myocardial infarction in the absence of treatment. Arch Intern Med 2002;162:2405–10.
Taylor RS, Brown A, Ebrahim S et al. Exercise-based rehabilitation for patients with coronary heart disease: systematic review and meta-analysis of randomized controlled trials. Am J Med 2004;116:682–92.
Cooper A, Skinner J, Nherera L et al. Clinical guidelines and evidence review for post myocardial infarction: secondary prevention in primary and secondary care for patients following a myocardial infarction. London: National Collaborating Centre for Primary Care and Royal College of General Practitioners, 2007.
Beswick AD, Rees K, Griebsch I et al. Provision, uptake and cost of cardiac rehabilitation programmes: improving services to under-represented groups. Health Technol Assess 2004;8:1–152.
Lane D, Carroll D, Ring C, Beevers DG, Lip GY. Predictors of attendance at cardiac rehabilitation after myocardial infarction. J Psychosom Res 2001;51:497–501.
Thompson RL, Summerbell CD, Hooper L et al. Dietary advice given by a dietitian versus other health professional or self-help resources to reduce blood cholesterol. Cochrane Database Syst Rev 2003;(3):CD001366.
Thompson RL, Summerbell CD, Hooper L et al. Relative efficacy of differential methods of dietary advice: a systematic review. Am J Clin Nutr 2003;77:1052S–1057S.
Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto miocardico. Dietary supplementation with n-3 polyunsaturated fatty acids and vitamin E after myocardial infarction: results of the GISSI-Prevenzione trial. Lancet 1999;354:447–55.
Quilici S, Martin M, McGuire A, Zoellner Y. A cost-effectiveness analysis of n-3 PUFA (Omacor) treatment in post-MI patients. Int J Clin Pract 2006;60:922–32.
Shuman J. Helping patients sort through the conundrum of dietary supplements. Primary Issues 2009;11:2–6.
National Institute for Health and Clinical Excellence. MI: secondary prevention. Costing report: Implementing NICE guidance. London: NICE, 2007.
Ranolazine has been evaluated in three trials in patients with stable angina (MARISA, CARISA and ERICA) and one large trial of patients with non-ST elevation acute coronary syndromes (MERLIN-TIMI 36). It has shown an improvement in exercise performance and a decrease in angina attacks. Ranolazine has similar efficacy in younger and elderly patients. Observational experience with ranolazine from a large UK centre is described.
Introduction
Coronary heart disease (CHD) remains the major cause of death throughout European and other developed countries. While death rates have been consistently falling, rates in the UK remain relatively high compared to some Western European countries. The commonest clinical presentation of CHD is angina pectoris. Angina incidence rates generally increase with age and are highest in the 65−74 years age group in both men and women. The prevalence of angina is estimated to be 5% in men and 4% in women in the UK, giving a total of nearly 2.1 million (>1.2 million <75 years of age) with the condition.1 It is therefore a common disease, which carries a prognosis similar to patients who have had a myocardial infarction (MI) or who have been revascularised.2 Many patients experience anginal attacks despite revascularisation and pharmacological antianginal treatments. In the Clinical Outcomes Utilization Revascularization and Aggressive Drug Evaluation (COURAGE) trial,3 for example, over 25% of patients experienced angina up to five years post-percutaneous coronary intervention (PCI) with optimal medical treatment (OMT). Such findings suggest that we need better strategies to improve both symptoms and prognosis in patients with chronic stable angina.
Ranolazine profile
This review looks at ranolazine, an antianginal which does not have a clinically significant effect on heart rate or blood pressure. Ranolazine is a piperazine derivative. Its molecular structure is shown in figure 1. It was approved by the US Food and Drug Administration in January 2006 as add-on therapy for the treatment of chronic angina and received a first-line indication in November 2008. The maximum approved dose in the US is 1,000 mg twice daily.
Figure 1. The molecular structure of ranolazine
In Europe, it was registered as Ranexa® (ranolazine prolonged-release tablets) in July 2008. Its approved indication is as add-on therapy for the symptomatic treatment of patients with stable angina pectoris who are inadequately controlled or intolerant to first-line antianginal therapies (such as beta blockers and/or calcium antagonists). The recommended initial dose in adults is 375 mg twice daily. After two to four weeks, the dose should be titrated to 500 mg twice daily. According to the patient’s response, it can be further titrated to the recommended maximum dose of 750 mg twice daily.
The mechanism of action is not fully elucidated but it is thought to be via selective inhibition of the late inward sodium current (INa) in cardiac muscle cells.4,5
This reduces intracellular sodium accumulation and calcium overload, and consequently improves myocardial relaxation and decreases left ventricular diastolic stiffness.6,7
Haemodynamic effects are minimal (decreases in mean heart rate <2 bpm and in mean systolic blood pressure <3 mmHg) in patients treated with ranolazine alone or in combination with other antianginal agents in controlled studies.8 Dose- and plasma concentration-dependent increases in the QTc interval (about 6 ms at 1,000 mg twice daily), reductions in T wave amplitude and notched T waves have been observed in patients treated with ranolazine. These effects are thought to relate to inhibition of the fast-rectifying potassium current. In the Metabolic Efficiency With Ranolazine for less Ischemia in Non-ST-Elevation Acute Coronary Syndromes (MERLIN-TIMI 36) study,9 there was a significantly lower incidence of arrhythmias among patients treated with ranolazine (74%) compared to placebo (83%), including ventricular tachycardias (5% vs. 8%). There has been no evidence of higher risk ‘torsade de pointes’ in clinical trials.
Pharmacokinetics
The mean bioavailability after oral administration of ranolazine varies from roughly 35 to 50%, and peak plasma concentrations are reached two to six hours after administration. Steady state is usually achieved within three days of twice-daily dosing. Trough concentrations occur about 12 hours after administration. Approximately 62% of ranolazine is bound to plasma proteins. It is eliminated primarily by metabolism (less than 5% is excreted unchanged). The terminal half-life at steady state after oral administration of ranolazine is about seven hours. Ranolazine undergoes rapid and extensive metabolism. In liver, ranolazine is metabolised principally by CYP3A4, but also by CYP2D6.
Clinical trials and drug efficacy
The development programme began with ranolazine immediate-release; later clinical trials used the sustained-release formulation. Some trials used doses of ranolazine which are outside the recommended doses but they have been included in this review for the sake of completeness. The Summary of Product Characteristics (SPC)10should be consulted for more comprehensive prescribing information.
The principal dose-response study was the Monotherapy Assessment of Ranolazine In Stable Angina (MARISA) trial,11 which randomised 191 patients. The main clinical study was the Combination Assessment of Ranolazine In Stable Angina (CARISA) trial,12 which included 823 patients; ranolazine 750 mg twice daily or 1,000 mg twice daily were added to atenolol, amlodipine or diltiazem. In a supportive study, the Efficacy of Ranolazine In Chronic Angina (ERICA) trial,13 565 patients were randomised to receive ranolazine 1,000 mg twice daily or placebo in addition to amlodipine 10 mg daily for six weeks. Finally, in the Metabolic Efficiency With Ranolazine for Less Ischemia in Non-ST-Elevation Acute Coronary Syndromes (MERLIN)-TIMI 36 trial, a total of 6,560 patients were randomised to receive ranolazine (initially intravenously [IV] and then 1,000 mg twice daily orally) or matching placebo within 48 hours of ischaemic symptoms. They were followed for a median of 348 days.
MARISA
The main dose-response study for ranolazine is the MARISA trial.11 The objectives of the trial were to assess the tolerability of three doses of ranolazine sustained-release compared to placebo and their effects on treadmill exercise performance.
Patients were at least 21 years old, with documented coronary artery disease and a history of at least three months of angina on effort. During the qualifying phase, prophylactic antianginal treatment was stopped and two modified Bruce exercise tolerance tests (ETTs) were conducted. Patients were randomised into the double-blind phase if they developed exercise-limiting angina and >1 mm ST segment depression during the ETTs.
The study was a double-blind, randomised, placebo-controlled, four-period crossover study. It enrolled 191 patients with stable angina: they received ranolazine SR at doses of 500 mg, 1,000 mg and 1,500 mg or placebo twice daily for one week. At the end of each treatment period, ETTs were performed four and 12 hours after dosing (these times approximate peak and trough plasma ranolazine concentrations). The primary efficacy end point was total exercise duration at trough. Other efficacy end points included time to onset of angina, time to 1 mm ST segment depression at trough, and the same ETT end points at peak.
Compared to placebo, treatment with ranolazine significantly improved total exercise duration: the mean difference at trough was 23.8 seconds for 500 mg twice daily, 33.7 seconds for 1,000 mg twice daily and 45.9 seconds for 1,500 mg twice daily, showing a clear dose-response pattern. The corresponding differences at peak were 29.3, 50.1 and 55.5 seconds, respectively.
Time to onset of angina, similarly, was longer with ranolazine than with placebo. At trough, the differences were 27.0, 45.9 and 59.6 seconds for ranolazine 500 mg, 1,000 mg and 1,500 mg twice daily, respectively. The time to 1 mm ST segment depression also improved against placebo, with trough value differences of 27.6, 44.5 and 64.6 seconds, respectively, for the three increasing doses of ranolazine. No clinically significant changes in rest or exercise heart rate or blood pressure were observed with ranolazine. In this study, exercise duration was longest in the 1,500 mg group; however, there was a disproportional increase in side effects and the 1,500 mg dose was not studied further.
A recent analysis from MARISA using exercise testing in 191 patients14 suggests that the progressive magnitude of ischaemia reduction on ranolazine was proportionally more substantial than minor reductions in heart rate or rate pressure product (RPP), suggesting ranolazine’s benefits may be due to an improvement in regional coronary blood flow in areas of myocardial ischaemia.
CARISA
The main clinical study of ranolazine in severe chronic angina is the CARISA trial.12 It was a randomised, three group, double-blind and placebo-controlled trial that enrolled 823 patients from 118 participating outpatient departments to receive placebo or one of two doses of ranolazine.
All patients had confirmed coronary artery disease and a history of at least three months of exertional angina. They were stratified according to the antianginal therapy that they were taking at enrolment (atenolol 50 mg, diltiazem 180 mg or amlodipine 5 mg daily). At the screening visit, patients had to have reproducible angina, ischaemic ST segment depression of at least 1 mm and limited exercise capacity on treadmill testing (three to nine minutes on a modified Bruce protocol). Eligible patients entered a single-blind qualifying phase during which they had two ETTs, conducted a week apart and each preceded by a 12-lead ECG. Subsequent exercise tests were performed at trough drug levels two, six and 12 weeks after randomisation. At two and 12 weeks after randomisation, a peak ETT was also performed four hours after dosing. The primary efficacy parameter was change from baseline in exercise treadmill time at trough. Angina frequency and nitroglycerin (NTG) consumption were also recorded.
The mean age was 64 years: fewer than 10% were aged 75 or older. About 23% were female. More than 60% were hypertensive and 58% had had a previous MI. Some 23% had diabetes. Patients were experiencing an average of 4.5 angina attacks per week; angina frequency and NTG consumption were similar across all groups. The patients were randomised to receive ranolazine 750 mg twice daily (n=279), 1,000 mg twice daily (n=275) or placebo (n=269) as add-on treatment to atenolol 50 mg once daily, amlodipine 5 mg once daily or diltiazem 180 mg once daily.
At baseline, all three treatment arms had an exercise duration of approximately seven minutes. Each individual ranolazine dose increased treadmill exercise duration at both trough (p=0.03) and peak (p<0.02). This effect was sustained throughout the 12 weeks of the study for both ranolazine doses, and similar results were observed for times to angina and ECG ischaemia.
At baseline, patients had approximately 4.5 angina attacks per week. Ranolazine reduced this number to 2.5 for the 750 mg twice-daily dose (p=0.006) and to 2.1 for the 1,000 mg twice-daily dose (p<0.001). It also reduced NTG consumption.
There was some concern about the robustness of these findings since baseline treatment was not maximised for all patients. A post hoc analysis of patients considered maximally dosed as a result of depressed heart rate, blood pressure and/or prolonged PR interval (n=249), showed similar results to those for the study population as a whole.18
ERICA
The ERICA trial studied ranolazine sustained-release in patients with stable angina who were also receiving conventional antianginal agents (here, the maximum recommended dose of amlodipine).13
For inclusion, patients were to be aged 18 years or over, with a documented history of coronary artery disease, chronic stable angina for three months or longer, and three or more angina episodes a week during the qualification period despite treatment with amlodipine 10 mg daily. Long-acting nitrates and sublingual NTG, as required, were permitted during the study period but other antianginal agents were not allowed.
Following a two-week qualifying phase, patients were randomised to receive ranolazine or placebo. During the initial one-week phase, patients received either ranolazine 500 mg twice daily or placebo; during the subsequent full-dose treatment phase, patients received either ranolazine 1,000 mg twice daily or placebo. Amlodipine 10 mg daily was continued throughout. Patients were evaluated at two weeks and six weeks after initiation of the full-dose phase to assess efficacy and the occurrence of adverse events.
The primary efficacy variable was the weekly average frequency of self-reported angina episodes during the six-week full-dose treatment phase. Secondary efficacy variables were average weekly NTG consumption during the six-week phase plus change from baseline of the five dimensions of the Seattle Angina Questionnaire (SAQ).
Some 565 patients were randomised; 98% of patients in each group completed the trial. Figure 2 shows patients receiving ranolazine had a significantly lower weekly rate of angina episodes compared with patients receiving placebo (trimmed mean 2.88 vs. 3.31, respectively). The average weekly rate of NTG consumption was significantly lower in patients receiving ranolazine during the treatment phase (p=0.014) though baseline NTG consumption did not differ between treatment groups.
Figure 2. The number of weekly angina attacks following treatment with amlodipine and ranolazine in the ERICA trial
The scores on the angina frequency dimension of the SAQ were significantly improved in patients receiving ranolazine (22.5 vs. 18.5) but the other SAQ dimensi ons were not significantly different between treatment groups. Subgroup analyses showed reductions of angina frequency and NTG use for those with a baseline frequency >4.5 per week, but only of angina frequency for those with fewer attacks at baseline.
Long-acting nitrates were used by 45% of the patients assessed. The treatment effect of ranolazine was consistent irrespective of gender, use of long-acting nitrates and age. Ranolazine had no clinically significant effects on heart rate or blood pressure.
Elderly patients
Age alone had no relevant effect on pharmacokinetic parameters. Pooled data from CARISA and ERICA15 indicate that the efficacy of ranolazine is similar in older (70 years or more) and younger patients but that adverse effects are more common in the elderly. The incidence of serious adverse effects attributable to ranolazine did not differ significantly between age groups. Cautious up-titration is needed in the elderly, who may have an age-related decrease in renal function.
UK observational experience
Whilst randomised clinical trials of antianginal agents, such as those above for ranolazine, have established their efficacy as first- or second-line agents, in actual practice newer agents are often used in a serial and additive manner on top of existing established therapy. Furthermore, they may be introduced into a patient population that is challenging to manage either because they continue to experience anginal symptoms despite conventional therapy, or in whom there are (multiple) drug intolerances. With six classes of antianginal agents, the utility and impact of adding a new drug for angina on top of several others is not well defined. Previous experience has also suggested a limited incremental benefit beyond two antianginal drugs.
In order to look at this issue further with respect to ranolazine, we recently conducted a retrospective analysis of a consecutive series of 25 patients in whom ranolazine had been prescribed. We examined GP and hospital records covering a mean of 27 months per patient spanning the period both before and after initiation of ranolazine.
The patient characteristics are summarised in table1. Most of these patients had advanced angina (Canadian Cardiac Society [CCS] Class III or IV) and more than half the patients had undergone at least one coronary revascularisation procedure. Prior to initiation of ranolazine, all of the patients had previously had coronary angiography undertaken to define the current extent of their coronary disease (including graft and/or stent patency) and the potential for further revascularisation. Importantly, many of the patients had undergone multiple coronary angiograms for recurrent chest pain and hospital admissions over the preceding years, suggesting a high burden of repeat angiographic investigations that did not result in revascularisation.
Table 1. UK observational experience with ranolazine
The mean number of other antianginal agents being taken by the patients prior to being prescribed ranolazine was 3.6 (range 2−5), with patients having tried an average of 4.2 (range 2−5) other antianginal agents (including those to which they were intolerant). Thus the data suggest that our use of ranolazine was often as a fourth-line agent in patients whose symptoms of chest pain were not controlled by multiple other antianginal drugs and in whom further revascularisation was not an option.
We sought to determine whether there was any subjective or objective evidence of antianginal benefit in this challenging patient group. Some 48% of patients reported a good symptomatic response following the initiation of ranolazine and a further 20% had at least some reduction in angina burden. A non-cardiac cause for the chest pain was subsequently diagnosed in half of the non-responders.
In the 18 months prior to initiation of ranolazine, there had been a mean of 3.96 admissions/patient for angina. Notably, the monthly hospital admission rate dropped by 54.5%, following commencement of ranolazine. Furthermore, only one patient (non-responder) went on to have repeat angiography and revascularisation. These observations are more striking when recalling that these patients had advanced angina and were already taking multiple antianginal agents. These data support a potentially useful role of ranolazine in reducing both symptoms and hospital admissions in some patients with difficult to control angina.
MERLIN-TIMI 36 study
The MERLIN-TIMI 36 trial was designed to evaluate the efficacy and safety of ranolazine as an intervention to reduce cardiovascular death, MI or recurrent ischaemia in the short and long term in acute coronary syndrome (ACS) patients at moderate to high risk who were already receiving standard therapy.9
It was a phase III, double-blind, parallel group, placebo-controlled trial that randomised 6,560 patients within 48 hours of ischaemic symptoms. Patients were randomised either to ranolazine 200 mg IV over one hour, followed by an 80 mg/h IV infusion for 12−96 hours, or to matching placebo. Once the infusion was completed, ranolazine extended-release 1,000 mg twice daily or matching placebo was instigated; patients were followed up for a median of 348 days.
The primary efficacy end point was the first occurrence of cardiovascular death, MI or recurrent ischaemia. Other secondary end points included failure of therapy (cardiovascular death, MI, recurrent ischaemia, positive findings on Holter monitoring for ischaemia, hospitalisation for heart failure or an early positive ETT). Quality of life was assessed by the SAQ. Safety end points included death from any cause, time to first occurrence of death from any cause or any cardiovascular hospitalisation, symptomatic documented arrhythmia, and clinically significant arrhythmia detected on Holter monitoring.
At baseline, 96.1% were being treated with aspirin and 90.3% with heparin. Median time from symptom onset to randomisation was 24 hours. Study drug was given intravenously to 6,541 patients (99.7%) for a median of 23 hours, and follow-up with oral administration of study drug took place in 6,399 patients (97.5%).
The composite primary efficacy end point occurred in 696 patients (21.8%) in the ranolazine group compared with 753 patients (23.5%) in the placebo group (hazard ratio [HR] 0.92, p=0.11). Failure of therapy occurred in 1,173 patients (36.8%) in the ranolazine group compared with 1,233 patients (38.3%) in the placebo group (HR 0.94, p=0.16).
Although ranolazine had no effect on the rate of cardiovascular death or MI, recurrent ischaemia was significantly lower in the ranolazine group (figure 3).
Figure 3. Graph showing recurrent ischaemia in the the MERLIN-TIMI 36 study
Recurrent ischaemia was defined here as: recurrent ischaemia with ECG changes, leading to hospitalisation or prompting revascularisation; or worsening angina by at least one Canadian Cardiovascular Society (CCS) class requiring intensification of therapy.
There was also a trend towards an early reduction in recurrent ischaemic complications (30-day cardiovascular death, MI, severe recurrent ischaemia, positive ischaemic changes on Holter monitoring) with ranolazine: this end point occurred in 23.1% of ranolazine patients and 25.1% of placebo patients, RR 0.92, p=0.055. Worsening angina by at least one CCS class was lower with ranolazine (4.2% vs. 5.9%, HR 0.77, p=0.02). An increase in antianginal therapy was less frequent in the ranolazine group (10.6% vs. 13.0%, HR 0.80, p=0.003). An improvement in angina frequency using the SAQ was recorded with ranolazine (p<0.001), particularly among patients who had a history of angina at study entry.
Effects on glycosylated haemoglobin
A post-hoc analysis of the CARISA trial examined the effect of ranolazine on glycosylated haemoglobin (HbA1c) in patients with diabetes.16 HbA1c values were obtained from 160/189 (85%) of patients at baseline and from 140/189 (74%) of patients with diabetes at 12 weeks. Ranolazine 750 mg and 1,000 mg twice daily reduced HbA1c compared with placebo by 0.48% (p=0.008) and 0.70% (p=0.0002), respectively. The reduction in HbA1c was greater among those patients receiving insulin. After adjusting for baseline differences, the percentage of patients with HbA1c <7% was significantly higher in the ranolazine 1,000 mg group (p=0.004). Levels of HbA1c appeared to remain unchanged beyond 12 weeks of ranolazine treatment in the long-term, open-label extension study (for up to two years).
A reduction in HbA1c was also observed in the MERLIN-TIMI 36 trial.17At four months, HbA1c fell from 7.5% to 6.8% with ranolazine, and 59% of patients with diabetes had reached the target HbA1c of <7%. Additionally, subjects without diabetes in the ranolazine group were 32% less likely to develop new hyperglycaemia, new increases in HbA1c >6% and new fasting glucose >110 mg/dL (p=0.003).
Safety and tolerability
For full recommendations on the use of ranolazine, prescribers are advised to consult the SPC.10 Ranolazine is generally well tolerated with undesirable effects generally being mild to moderate in severity and often developing within the first two weeks of treatment.10
The most common adverse events reported in patients receiving ranolazine in the phase 2/3 chronic angina programme were constipation, nausea and asthenia. The incidence of adverse events leading to study discontinuation was 6.3% for ranolazine-treated patients compared with 3.0% for placebo-treated patients.18 In the dose-finding MARISA study, increasing the dose from 1,000 mg twice daily showed a disproportionate increase in the most frequent adverse events. Furthermore, early withdrawal from the study because of adverse events also occurred more frequently during dosing with 1,500 mg twice daily.11 As a result, this higher dose was not studied further; within the therapeutic range, ranolazine is generally well tolerated.
Some 746 patients who completed the MARISA or CARISA trial participated in the Ranolazine Open Label Experience (ROLE).19 Two years after initial dosing, 571 patients (76.7%) remained on therapy, and 72 patients (9.7%) discontinued ranolazine due to adverse events. Some 64 deaths occurred during a total of 2,102 patient years (3.0% annually). Such survival analyses suggest that symptomatic improvements attributable to ranolazine are not offset by increased mortality.19
In healthy volunteers and chronic angina patients, treatment with ranolazine was associated with small dose-related mean increases in QTc from baseline.18 In the pivotal clinical studies, mean changes from baseline in QTcF (Fridericia’s correction) after doses of 500 mg and 750 mg twice daily were 1.9 and 4.9 ms, respectively.10 However, in the trial programme there has been no evidence of an increased risk of torsades de pointes.18 No proarrhythmic effects were observed in 3,162 patients treated with ranolazine based on seven-day Holter monitoring in the MERLIN-TIMI 36 study. There was a significantly lower incidenced of arrhythmias in patients treated with ranolazine versus placebo, including ventricular tachycardia ≥ 8 beats.10
Ranolazine is contraindicated in patients with severe renal impairment (with creatinine clearance <30 ml/min). A 1.3- to 1.8-fold increase in ranolazine exposure is estimated to occur in these patients. It is contraindicated in patients with severe or moderate hepatic impairment. In moderate impairment, the ranolazine ‘area under curve’ (AUC) was increased 1.8-fold, and QT prolongation was more pronounced.10 Contraindications with other drugs are discussed below.
Drug interactions
Inhibitors of CYP3A4 increase plasma concentrations of ranolazine and hence increase the potential for dose-related adverse events such as dizziness and nausea. The concomitant administration of ranolazine with potent CYP3A4 inhibitors (itraconazole, ketoconazole, voriconazol, posaconazol, HIV protease inhibitors, clarithromycin, telithromycin and nefazodone) should be avoided. Grapefruit juice is also a potent inhibitor of CYP3A4. Caution is recommended in combining ranolazine with moderately potent CYP3A4 inhibitors including diltiazem, erythromycin and fluconazole. Initiation of treatment with ranolazine should be avoided in those receiving CYP3A4 inducers e.g. rifampicin, phenytoin.
Simvastatin metabolism and clearance are highly dependent on CYP3A4. Ranolazine 1,000 mg twice daily increased plasma concentrations of simvastatin lactone, simvastatin acid, and the HMG-CoA reductase inhibitor activity by 1.4- to 1.6-fold.
Co-administration of Class Ia (such as quinidine) or Class III (such as dofetilide and sotalol) antiarrhythmics other than amiodarone is contraindicated.
There is a theoretical risk that co-administration of ranolazine with other drugs known to prolong the QTc interval may cause an interaction that increases the risk of ventricular arrhythmias e.g. the antihistamines, terfenadine, astemizole and mizolastine; the antiarrhythmics, quinidine, disopyramide and procainamide; erythromycin; and the tricyclic antidepressants, imipramine, doxepin and amitriptyline.
Conclusions
Ranolazine is an antianginal with a non-haemodynamic mechanism of action. It is used as adjunctive therapy in patients with chronic stable angina whose angina is uncontrolled adequately with conventional treatment such as beta blockers and rate-limiting calcium antagonists. Randomised clinical trials show that the drug improves exercise performance, decreases angina and nitrate consumption, compared to placebo. Observational experience suggests that ranolazine response rates are encouraging in more therapeutically challenging patients after revascularisation and in the presence of multiple other antianginal medications. It is comparatively well tolerated with little effect on haemodynamics or cardiac conduction, apart from a modest increase in QT interval, which is not clinically compromising. Ranolazine has potential use in a number of other cardiovascular conditions20 but presently it offers a useful alternative and adjunct to conventional antianginals in selected patients with chronic stable angina.
Conflict of interest
KK has received fees for advisory services with A Menarini Pharma, UK SRL, manufacturers of ranolazine. He does not hold stock in the company. MJ: none declared.
Editors’ note
Menarini has reviewed this article before publication for medical accuracy only. Full editorial control of this article resides with the authors and the journal.
Key messages
Ranolazine is indicated at doses of up to 750 mg twice daily as an add-on treatment for angina pectoris patients with inadequately controlled symptoms or who are intolerant to first-line antianginals
It does not depend on reductions in heart rate or blood pressure for its antianginal effects
It is reasonably well tolerated, it increases exercise time duration, reduces angina attacks and nitrate consumption versus placebo
References
Scarborough P, Bhatnagar P, Wickramasinghe K, Smolina K, Mitchell C, Rayner M. Coronary heart disease statistics 2010. British Heart Foundation 2010.
Buckley B, Murphy AW. Do patients with angina alone have a more benign prognosis than patients with a history of acute myocardial infarction, revas-cularisation or both? Findings from a community cohort study. Heart 2009;95:461–7.
Boden W, O‘Rourke R, Teo K et al. Optimal medical therapy with or without PCI for stable coronary disease: the COURAGE trial. N Engl J Med 2007;356:1503–-16.
Antzelevitch C, Belardinelli L, Zygmunt AC et al. Electrophysiological effects of ranolazine, a novel antianginal agent with antiarrhythmic properties. Circulation 2004;110:904–10.
Song Y, Shryock JC, Wu L et al. Antagonism by ranolazine of the pro-arrhythmic effects of increasing late INa in guinea pig ventricular myocytes. J Cardiovasc Pharmacol 2004;44:192–9.
Belardinelli L, Antzelevitch C, Fraser H. Inhibition of late (sustained/persistent) sodium current: a potential drug target to reduce intracellular sodium-dependent calcium overload and its detrimental effects on cardiomyocyte function. Eur Heart J 2004;6(suppl A):A13–17.
Hayashida W, van Eyll C, Rousseau MF et al. Effects of ranolazine on left ventricular regional diastolic function in patients with ischemic heart disease. Cardiovasc Drug Ther 1994;8:741–7.
European Medicines Agency.CHMP Assessment Report for Latixa European Medicines Agency Evaluation of Medicines for Human Use, 2008. Doc Ref: EMRA/CHMP/30876/2008.
Morrow DA, Scirica BM, Karwatowska-Prokopczuk E et al for the MERLIN-TIMI 36 Trial Investigators. Effects of ranolazine on recurrent cardiovascular events in patients with non-ST-elevation acute coronary syndromes. The MERLIN-TIMI 36 Randomized Trial. JAMA 2007;297:1775–83.
Chaitman BR, Skettino SL, Parker JO et al, for the MARISA Investigators. Anti-ischemic effects and long-term survival during ranolazine monotherapy in patients with chronic severe angina. J Am Coll Cardiol 2004;43:1375–82.
Chaitman BR, Pepine CJ, Parker JO et al for the Combination Assessment of Ranolazine In Stable Angina (CARISA) Investigators. Effects of ranolazine with atenolol, amlodipine, or diltiazem on exercise tolerance and angina frequency in patients with severe chronic angina. A randomized controlled trial. JAMA 2004;291:309–16.
Stone PH, Gratsiansky NA, Blokhin A, Huang I-Z, Meng L, for the ERICA Investigators. Antianginal efficacy of ranolazine when added to treatment with amlodipine: the ERICA (Efficacy of Ranolazine in Chronic Angina) Trial. J Am Coll Cardiol 2006;48:566–75.
Stone PH,Chaitman BR, Stocke K. The anti-ischemic mechanism of action of ranolazine in stable ischemic heart disease. J Am Coll Cardiol 2010; 56:934–42.
Rich MW, Crager M, McKay CR. Safety and efficacy of extended-release ranolazine in patients aged 70 years or older with chronic stable angina pectoris. Am J Geri Cardiol 2007;16:216–21.
Timmis AD, Chaitman BR,
Crager M. Effects of ranolazine
on exercise tolerance and HbA1c in patients with chronic angina and diabetes. Eur Heart J 2006; 27:42–8.
Morrow DA, Scirica BM, Chaitman BR, et al. Evaluation of the glycometabolic effects of ranolazine in patients with and without diabetes mellitus in the MERLIN-TIMI 36 randomised controlled trial. Circulation 2009;119:2032–9.
Koren M, Crager M, Sweeney M. Long-term safety of a novel antianginal agent in patients with severe chronic stable angina, The Ranolazine Open Label Experience (ROLE). J Am Coll Cardiol 2007;49:1027–34.
Chaitman B. Ranolazine for the treatment of chronic angina and potential use in other cardiovascular conditions. Circulation 2006;113:2462–72.
You are not logged in
You need to be a member to print this page.
Find out more about our membership benefits
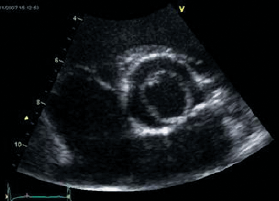
 (a) and first septal branch (b). Also noted is a temporary pacing wire in the right ventricular apex (c), pigtail catheter (d) in the left ventricular cavity and guide catheter engaged in the left coronary artery (e). B. An over-the-wire balloon is then inflated in the septal branch and the guidewire removed")
 in the apical four-chamber view and shown to perfuse the proximal septum confirming that the septal branch is supplying the target area for alcohol ablation")
")
")

 classification at baseline (n=15) and more than nine months (n=13) after alcohol septal ablation")




 and trans-oesophageal (C) echocardiography showing the presence of a large nodular free-floating left atrial thrombus along with a nodular thrombus attached to anterior mitral valve leaflet (arrow heads) in a patient with rhupus and secondary antiphospholipid syndrome")






 assessment")



")

 in the UK")




