Released 1 March 2016 Expires: 01 March 2018 Programme: Heart valve disease1 CPD/CME credit
Sponsorship Statement: This module has been sponsored by Edwards Lifesciences with an unrestricted educational grant
Designed to give healthcare professionals an understanding of the causes and frequency of heart valve disease. It is one of several modules in our heart valve disease programme.
1 CPD/CME credit
Module originally published May 2013. Revised module released March 2016
Learning objectives
Upon completing this module, participants should be better able to:
Understand the temporal and geographical trends in valve disease
Understand the prevalence and incidence of valve disease
Understand the causes of valve disease by position
Be aware of variations in access to care.
Faculty
Professor John Boyd Chambers, St Thomas’ Hospital, London
Accreditation
1 CPD/CME credit, 1 hour
BJC Learning has assigned one hour of CPD/CME credit to this module
The European Board for Accreditation in Cardiology (EBAC) has assigned one CME credit to this module. German participants should contact EBAC to receive a German VNR code for this course. email:accreditation@ebac-cme.org website: http://www.ebac-cme.org/
You need to be a registered member to view this page. It's quick, free and offers you a host of other benefits, including the facility to print and download articles and supplements, access our archived issues and receive email updates when new issues and other content are online.
Transcatheter approaches to the mitral and aortic valves offer an alternative therapeutic strategy currently reserved for patients with a predicted high surgical mortality. This module focuses on recently approved devices, as well as investigational approaches to mitral and aortic valve reconstruction.
Dr Alain Cribier, pioneer of transcatheter aortic valve implantation
The background to transcatheter aortic valve implantation (TAVI) was recently reviewed in a TAVI-focus issue of the European Heart Journal.1 In a search for less invasive treatment methods, the concept of transcatheter implantation of heart valves was pioneered by Henning Anderson for the aortic, and Philipp Bonhoffer for the pulmonary position, followed by the first percutaneous human implantation of an aortic valve prosthesis by Alain Cribier in 2002. The Food and Drug Administration (FDA) approved the SAPIEN valve in November 2011 for the treatment of inoperable patients, and expanded the indication to high-risk surgical patients in October 2012. Over the past decade the treatment of severe aortic stenosis has been revolutionised with over 10,000 TAVI procedures being performed.
Aortic valve replacement
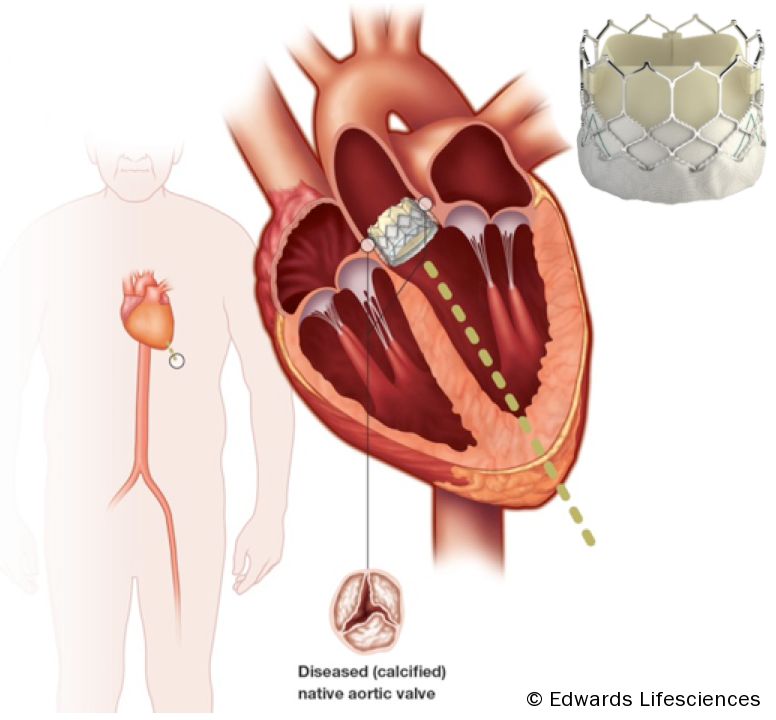
The basic concept of the transcatheter aortic valve replacement devices involves delivering a stented trileaflet bioprosthetic valve to the site of the diseased native valve, either via a transfemoral, transapical, or direct aortic approach (see figure 1).
Figure 1. Transcatheter aortic valve replacement devices. Edwards SAPIEN transcatheter heart valve, RetroFlex 3 delivery system and Ascendra balloon catheter delivery system
Patient selection
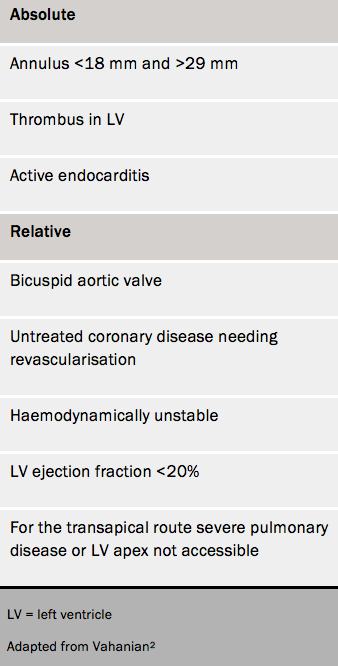
Table 1. Contraindications for TAVI (ESC guidelines)
TAVI is indicated for symptomatic severe aortic stenosis when the ‘heart team’ at a cardiac surgical centre has determined that the patient:
Is unsuitable for conventional surgery because of severe comorbidities
Is likely to have an improvement in quality of life as a result of the intervention
Has a life expectancy of at least one year.
The calculation of risk is difficult since no wholly satisfactory score exists. A combination of surgical scores and a frailty index should be used and it is important to have specialists in elderly care involved in the decision.
If the estimated surgical risk is not high, the heart team may still decide that TAVI is preferable to conventional surgery for individual reasons including frailty, prior chest irradiation, porcelain aorta. Its use in intermediate-risk and lower risk patients is discussed later.
Contraindications for TAVI are given in table 1.2,3
Surgery in left-sided valve heart disease (mitral and aortic valves) is usually indicated for significant valve disease associated with either symptoms or with evidence of left ventricular dysfunction (figure 1).
Surgery is indicated for mitral stenosis, with a raised pulmonary artery (PA) pressure before right ventricular (RV) dysfunction develops. Criteria for surgery are provided by European Society of Cardiology (ESC) and American Heart Association (AHA) guidelines which are similar.1,2
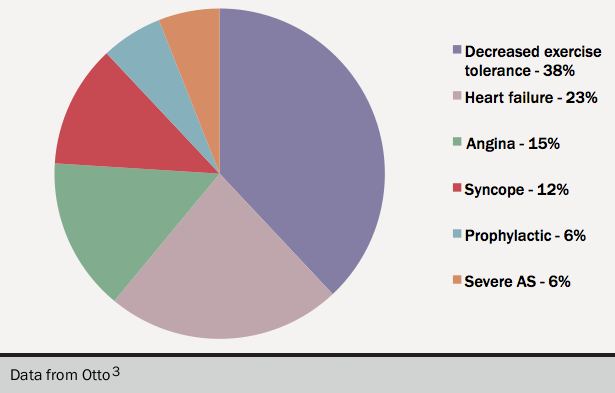
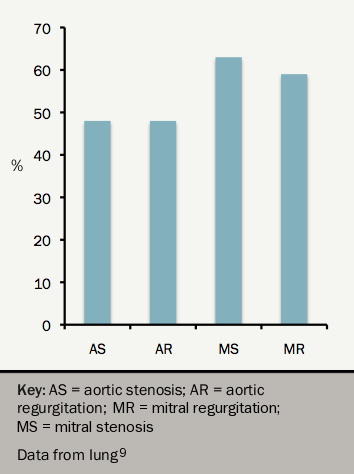
Figure 2. Criteria for surgery in 48 patientsFigure 3. Proportion of NYHA III/IV at surgery
As patients slow down to avoid symptoms (figure 23) exercise testing should be considered in all patients at low risk for surgery, to confirm that they are truly asymptomatic.
For all heart valve disease patients a combination of symptoms and severe disease is a class I indication for surgery.
Surgery, when indicated, should be performed at the start of mild but definite symptoms. The risk of surgery doubles with severe symptoms and recovery is slower. In the EuroHeart survey 50% of all patients having surgery were in New York Heart Association (NYHA) Class III or IV (figure 34).
This module will describe indications for surgery according to the valve affected. The module will not cover the techniques of conventional heart valve surgery. However the video below provides coverage of an open chest heart valve replacement operation. Module 10 covers aspects of transcatheter aortic valve implantation (TAVI) and transcatheter mitral techniques.
For those wishing to read about heart valve surgery in general, the following text is recommended:
Oxford Specialist Handbooks in Surgery – Cardiothoracic Surgery
Authors: Joanna Chikwe, David Tom Cooke, Aaron Weiss
Second Edition- ISBN 978-0-19-964283-0
Published by: Oxford University Press (www.oup.com)
Great Clarendon Street, Oxford OX2 6DP
First Edition published in 2006. Second Edition published in 2013
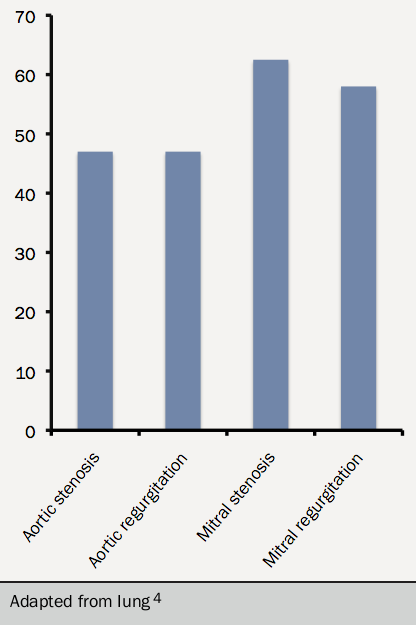
Infective endocarditis (IE) is uncommon but important because it is difficult to manage and universally fatal unless appropriately treated. The estimated incidence is 3–10 episodes per 100,000 population each year,1 and this is gradually rising although the reasons for the increase are not known.2,3 Most cardiothoracic centres see between 50–100 cases per year.2
The epidemiology of IE is changing.4 In industrially developed countries, increasing numbers result from infection of pacing devices, replacement heart valves and medical interventions such as haemodialysis.
The average age of patients with IE is increasing4 but younger age-groups are also affected, particularly intravenous drug users (IVDU) and those with adult congenital heart disease.5 Predisposing factors include diabetes, cancer and haemodialysis.6
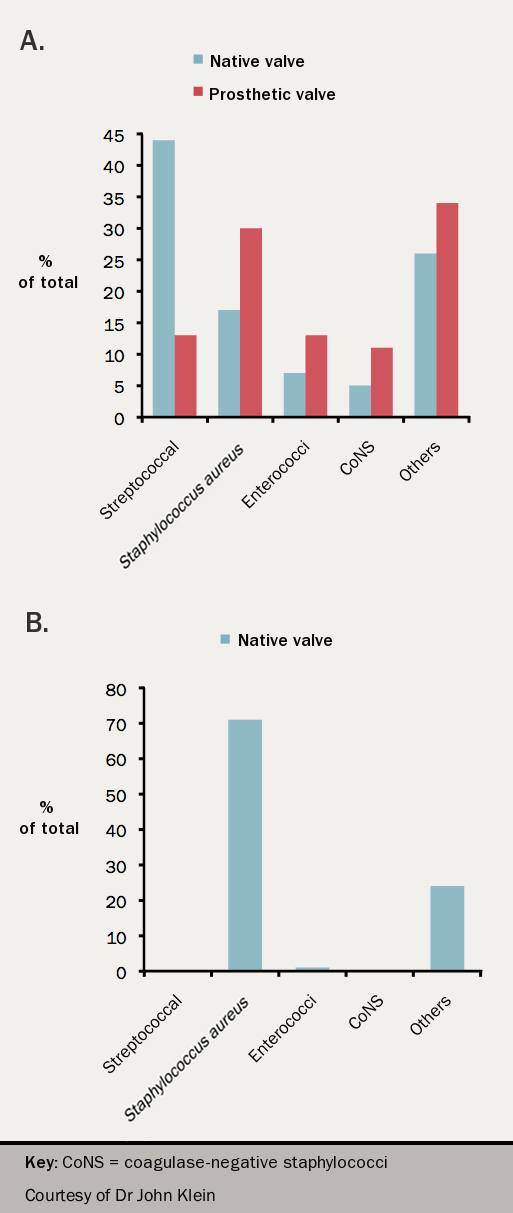
Figure 1. Histogram of frequencies of organism 1970–2005 at St Thomas Hospital in A) native and prosthetic valve endocarditis, and B) intravenous drug use
The most common organisms causing native valve IE in non IVDU are the oral streptococci followed by staphylococci and enterococci (see figure 1) while in IVDU the predominant organism is Staphylococcus aureus. After device implantation, prosthetic valve or pacemaker, staphylococci predominate (both S aureus and coagulase negative staphylococci (CNS)). Late prosthetic valve endocarditis (occurring one year after surgery) is most often caused by oral streptococci.
In-hospital mortality is high, about 20%7 and is associated with:
delayed diagnosis,
prosthetic valve involvement,
increasing age,
heart failure
staphylococcal infection.6,7
When to suspect IE
It should be suspected if there is:
Fever with underlying structural heart disease or intracardiac device
Fever and new murmur of valve regurgitation
Fever with vasculitic lesions or stroke
A suspicious organism in blood cultures (e.g. S. aureus or community acquired Enterococcus faecalis) or persistently positive blood cultures
A splenic infarct(s)/abscess or haematogenous spinal infection or brain abscess
Staphylococcus aureus bacteraemia related to a line but only if the fever fails to settle within 48 hours or blood cultures remain positive after 72 hours or there are emboli or other features suggestive of IE
Both native valve disease and prosthetic valves may increase the risk of embolic stroke and systemic embolism. This section will address which patients require antithrombotic treatment and what regimes to use.
Antithrombotic options
Figure 1. Warfarin can reduce but not eliminate the risk of thromboembolism
There are two main therapies used to anticoagulate patients with heart valve replacement. This is either with a heparinoid or a vitamin K antagonist. The use of non-vitamin K oral anticoagulants (NOACs) in valvular heart disease and in those with heart valve replacements has become increasingly popular but data on their long term safety and efficacy are awaited. This is covered in a separate section.
Vitamin K antagonists
Anticoagulation with vitamin K antagonists (VKA), such as warfarin, can reduce but not eliminate the risk of thromboembolism (see figure 1). They carry a substantial bleeding risk. The balance between risk and benefit must be carefully considered in every patient, particularly when valvular surgery is planned. The risk of bleeding on warfarin increases with age. Mechanical heart valves are more durable than prosthetic heart valves and life long anticoagulation is required due to the thrombogenicity of the valve. In addition, the incidence of thromboembolism is highly dependant on other factors, such as valve design and patient related risk factors.1 The risk of valvular thromboembolism is estimated at 0.2−1.5% per year and the risk of major bleeding to be around 1–2.5% per year.
Heparinoids
Intravenous unfractionated heparin (UFH) is suitable for short-term anticoagulation such as at the initiation of anticoagulation or when it has to be interrupted for invasive procedures. It is not suitable for long-term anticoagulation since inpatient monitoring of APTT ratio is required. Prolonged use of subcutaneous UFH is associated with osteoporosis and therefore not recommended as long-term therapy.
Low molecular weight heparins (LMWH) are not licensed at the current time for valvular heart disease but are extensively used short term as an alternative to UFH and offer effective and stable anticoagulation. This is, however, an off-label use and there is a lack of randomised control trials comparing its safety and efficacy against warfarin. In addition, there are ongoing concerns regarding its pharmacokinetics in patients of extreme body habitus (body mass index <15 and >25) and also the lack of specific antidote. The current European Society of Cardiology (ESC)/European Association for Cardiothoracic Surgery (EACTS) guidelines recommend anti-Xa monitoring if LMWH heparin is used.
Antiplatelet agents
Antiplatelet drugs are not an adequate substitute for anticoagulation with VKA where this is specifically indicated, but may be useful for reducing risk in patients with incidental valve disease who have other vascular risk factors, in the absence of a clear indication for anticoagulation. Aspirin may also be considered as an adjunct to VKA in some patients who have embolic events despite good anticoagulant control.
Native valve disease
Rheumatic mitral valve disease
This carries a substantial thrombotic risk. Patients may present with a systemic embolism as the first manifestation of the disease. Anticoagulation with VKA to a target INR of 2.5 is indicated in the presence of:
Previous systemic embolism
Atrial fibrillation (AF), persistent or paroxsysmal
Left atrial thrombus.
Anticoagulation should also be considered when there is significant left atrial enlargement in the absence of the above features. The presence of left atrial thrombus that does not resolve with anticoagulation is a contraindication for percutaneous mitral valvotomy.
Other valve disease
Mitral valve prolapse and mitral ring calcification are not in themselves indications for anticoagulation. Aortic, tricuspid or pulmonary valve disease do not carry such a high risk of thromboembolism as rheumatic mitral valve disease, and anticoagulation with a VKA is not indicated unless there are other complications such as AF.
The management of valve disease can be divided into three main steps:
(1) Detection.
(2) Planned management including surveillance.
(3) Appropriate surgery or percutaneous intervention.
There is broad agreement that limitations exist at all levels. This module discusses these and the evidence for methods of improving care.
Detection
The prevalence of moderate or severe heart valve disease using echocardiographic screening of populations is 2.5%.1 This compares with 1.8% using echocardiography only when clinically indicated. Severe aortic stenosis causes approximately one unexpected death at the time of major non-cardiac surgery per Trust per year in the UK.2
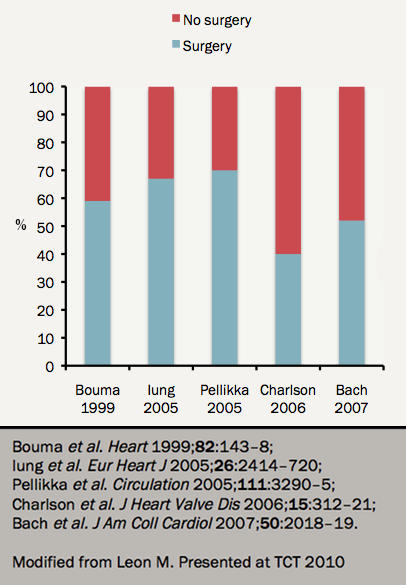
Figure 2. Severe AS: >30% not referred for surgery
Community screening by echocardiography can increase detection rates by a factor of up to 10,3 but this includes mild disease. While detecting mild rheumatic disease leads to important secondary prophylaxis, the gain is less evident for other types of disease since there is no proven means of reducing the rate of progression. There is, however, some evidence for the need to control modifiable risk factors.4 A proportion of patients progress to severe disease in five years5 making it clinically appropriate to recommend surveillance to allow optimal timing of surgery.
Medical management and surveillance
Limitations
The initial management of patients with valve disease is usually conservative.6,7 Meticulous follow-up at an interval appropriate to the level of valve disease is then vital. However accepted management guidelines are not followed adequately. In a Canadian study8 the rate of adherence to American Heart Association (AHA) guidelines varied between only 2% and 30% and adherence is also limited in the USA, Europe9 and the UK.10
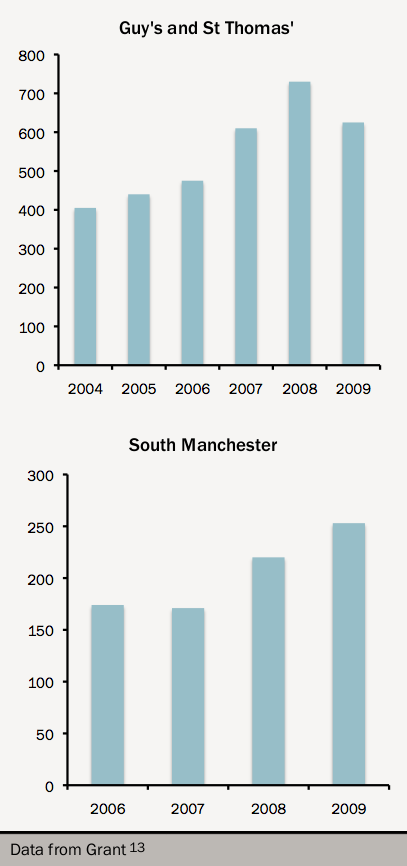
Figure 3. Effect of TAVI programme on surgical activity
As a result, patients are often referred for surgery too late. In the EuroHeart Survey,9 around one half with valve disease were in NYHA Class III or IV at the time of surgery (see figure 1).
At least one third (range 30–60%) of elderly patients with severe aortic stenosis are not referred for surgery at all even when clinically indicated11,12 (see figure 2). The development of a percutaneous valve programme leads to increased rates of conventional surgery13 suggesting that there were clinically inappropriate perceptual barriers to referral (see figure 3).
Patients with normally-functioning replacement valves should be assessed clinically every year,6,7 but may not require regular echocardiography. In practice, these patients are often discharged to their primary physician.
In this module, we will cover medical therapy for the treatment of valvular heart disease (VHD). Pharmacotherapy of VHD can be divided into two broad areas – supportive treatment and disease-modifying treatment. With the exception of a number of large-scale clinical trials in patients with aortic stenosis, we must rely on small studies and expert opinion. We will discuss medical therapy for the major valvular lesions, indications for anticoagulation in native valve disease, and finally examine recommendations for endocarditis prophylaxis – an area that has seen major changes in guidelines over the past decade.
Aortic stenosis
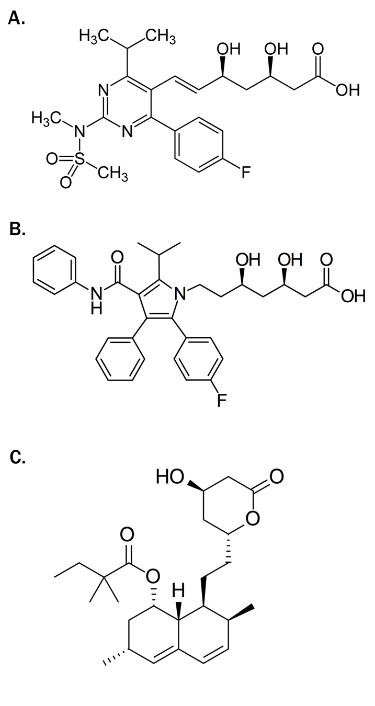
Figure 1. Chemical structure of commonly used statins. Panel A) rosuvastatin; panel B) atorvastatin; panel C) simvastatin
With the growing evidence that calcific aortic stenosis (AS) is not a “degenerative” process, but rather a process heavily influenced by inflammation, fibrosis, and subsequent calcification came the search for potential medical therapies to halt (or at least slow) progression of the disease. Similarities between the lesions of aortic stenosis and atherosclerosis, high crossover of risk factors amongst those developing atherosclerosis and AS, and results from observational studies and experimental models led to a number of large scale trials examining the role of statin therapy in AS.1–3
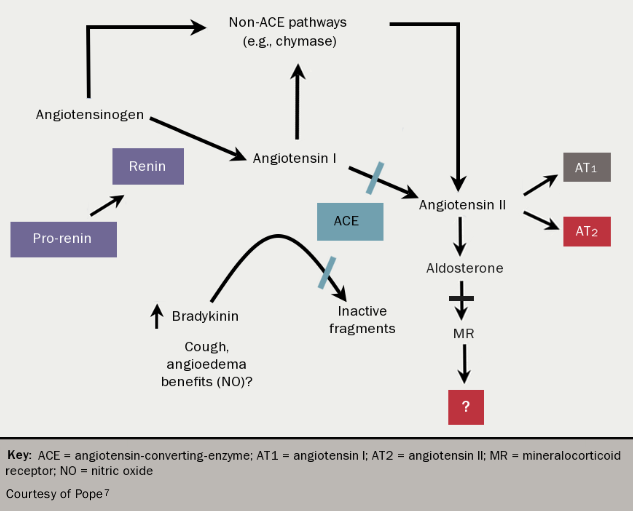
Unfortunately, these trials uniformly showed that statins (see figure 1) do not affect the progression of AS, although a reduction in ischaemic cardiovascular endpoints was seen in the largest study.2 This is likely to reflect the fact that whilst similar, the two atherosclerotic disease processes have important differences, perhaps most notably the advanced calcific response observed in the aortic valve. Strategies targeting calcification directly may be most likely to prove successful. For example, bisphosphonates reduce vascular calcification in experimental settings and these agents may therefore have beneficial effects within the aortic valve. Other potential disease modifying therapies are angiotensin converting enzyme inhibitors (ACEIs) and angiotensin receptor blockers (ARBs), as the renin-angiotensin-aldosterone system (RAAS) is upregulated at valve level in AS4 and beneficial effects have been seen with these agents in animal studies.5,6 (see figure 27). Population-based studies have shown improved outcomes in patients with all degrees of severity of AS using ACEIs and ARBs.8 However, in the Losartan Intervention for End Point Reduction in Hypertension (LIFE) study, neither the ARB losartan nor the beta blocker, atenolol, prevented the progression of aortic valve sclerosis.9
An alternative therapeutic approach may be to protect the myocardium from the effects of pressure overload in AS. For example, RAAS modulators and beta-blockers may exert beneficial effects by slowing the development of myocardial interstitial fibrosis, a marker of worse prognosis after aortic valve replacement (AVR),9 through down-regulation of transforming growth factor beta (TGF-β).10 Disappointingly, a trial of the aldosterone antagonist eplerenone in 65 patients did not show any benefit with regards to either disease progression or change in left ventricular function.11 However, the recent Ramipril in Aortic Stenosis (RIAS) trial randomised 100 patients with moderate or severe AS to ramipril or placebo, with a primary (non-clinical) endpoint of altered left ventricular mass over 12 months.12 There was a small but statistically significant difference in left ventricular mass in those allocated ramipril treatment, and a further trial examining the effect of ramipril on reduction of clinical endpoints is now planned.
Figure 2. The renin angiotensin aldosterone system
The mainstay of diagnosis in heart valve disease is imaging, using transthoracic echocardiography.1,2 This module describes the information required from echocardiography to diagnose heart valve disease and inform decisions about further management. It also discusses the complementary information available from cardiac magnetic resonance (CMR) and computed tomography (CT) imaging.
Aortic stenosis
The minimum echocardiographic data set
The echocardiographic minimum dataset for aortic stenosis consists of:
a detailed description of the valve appearance and mobility
Doppler parameters including peak velocity, mean gradient, and effective orifice area (EOA) calculated using the continuity equation:3,4
pulmonary artery pressure and right ventricular function.
Grading on echocardiography
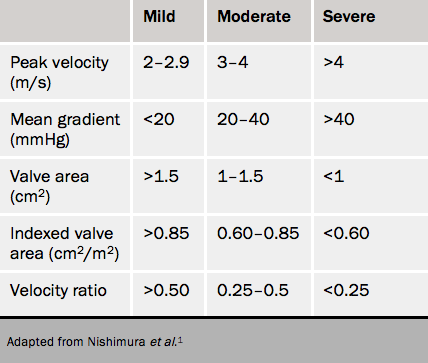
Table 1. Severity grading of aortic stenosis1
The cut-offs for grading can be found in table 1. Discrepancies are common and are usually caused by:
incorrect measurements
high or low flow
extremes of body size.
In addition, there is evidence that in European populations the cut-off maximum velocity (V max) of 4.0 m/s and mean gradient 40 mmHg coincide better with an EOA of 0.8 cm2 rather than 1.0 cm2.
The first step is to check measurements:
Is the LV outflow diameter too small? This can occur if there is a prominent subaortic septal bulge. Take the diameter at or close to the echocardiographic annulus at the base of the cusps.
There is recent data showing that the LV outflow tract may be oval rather than circular in cross-section in some patients. The continuity equation can be corrected by measuring the area directly using 3D echocardiography or CT. Check that the pulsed sample has been placed in the LV outflow tract just apical to the valve where the colour starts to alias. Pacing this too apical will cause an erroneously low effective orifice area.
Has continuous wave been recorded using a stand-alone probe from at least apical and right intercostal windows?
The key to resolving the discrepancies is to look at the valve and the waveform shape.
Severe area (<1.0 cm2) and moderate gradient (mean <40 mmHg)
The most common situation is an EOA of about 0.9 cm2 with V max 3.5–3.9 m/s in the presence of apparently normal LV systolic function. If the waveform is dagger-shaped and the valve opens well, this is moderate aortic stenosis (AS).
It can also help to index EOA to body surface area (BSA) (see table 1). An EOA of 1.3 cm2 (apparently moderate) in a small person (BSA 1.5 m2) gives an effective orifice area index (EOAi) of 0.86 cm2/m2 (mild AS), while in a big person (BSA 2.5 m2) the EOAi is 0.52 cm2/m2 (severe AS).
If the valve does not open well, look at the LV and check the velocity-time integral (VTI). If the ejection fraction (EF) is <40% or the VTI is low (<15 cm), this is low flow AS.5 A stress echocardiogram (see figure 1) should be considered.
Figure 1. Low left ventricular ejection fraction aortic stenosis
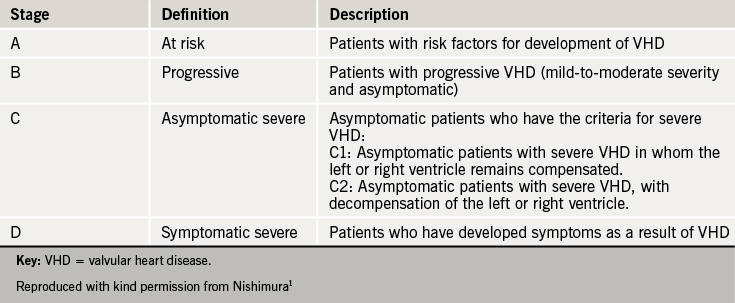
The clinical presentation of heart valve disease (HVD) varies widely, even for the same lesion of similar severity. The natural history of HVD is not well elucidated, although studies have been able to identify some high-risk features. Patients with HVD may present with mild or more advanced symptoms and signs, ranging from a subtle heart murmur to overt heart failure, or with incidental evidence of valvular abnormality on thoracic imaging by different modalities. Irrespective of the valve involved, presentation can occur at any stage of the disease, and the natural history is a progressive one. The recent American Heart Association (AHA)/American College of Cardiology (ACC) guidelines1) place greater emphasis on the progression of HVD, and suggest a four stage classification of HVD (see table 1) to better describe the whole spectrum and continuity of the disease.
Table 1. Stages of progression of valvular heart disease from the AHA/ACC guidelines
This module describes what is known of the natural history of individual lesions, along with the symptoms and signs of each lesion.
Aortic stenosis
Natural history
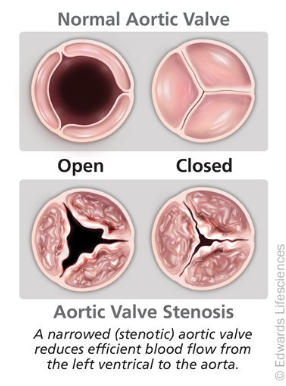
Figure 1. Normal and stenotic valves
Aortic stenosis (AS) is gradually progressive (see figure 1) and patients may remain asymptomatic for many years,2,3 even with severe stenosis. Typically symptoms develop above the age of 65 in those with calcific disease. However, bicuspid aortic valves are subject to abnormal shear stresses, resulting in earlier leaflet thickening and calcification. Intervention is required, typically between the ages of 50 and 70 years.4,5
In industrially underdeveloped regions of the world, rheumatic AS (see figure 2) tends to result in symptoms between 20 and 50 years of age. However, calcified rheumatic valves are still found in the elderly in industrialised countries.
The annual rate of progression of aortic stenosis is, on average:
A peak velocity increase by 0.3 m/s
Mean pressure gradient increase by 8 mmHg6–10
Effective orifice area fall by 0.1 cm2
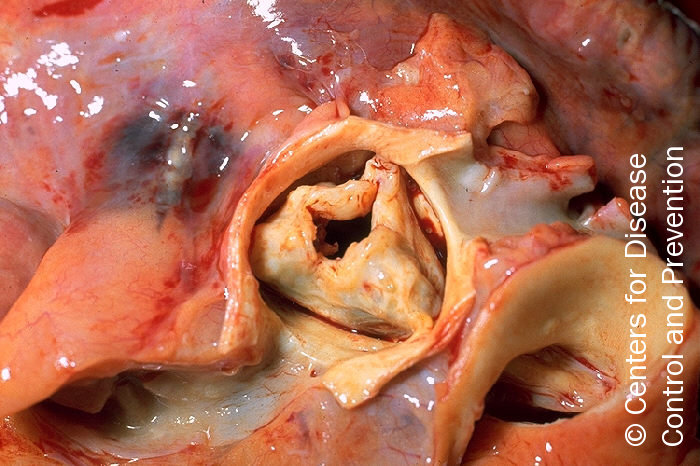
Figure 2. Gross pathology of rheumatic heart disease: aortic stenosis. Aorta has been removed to show thickened, fused aortic valve leaflets and opened coronary arteries from above
Asymptomatic severe AS has low morbidity and mortality, with a risk of sudden death of approximately 1% per year. Survival rates in those declining surgery for severe symptomatic AS are between 15% and 50% at five years. More severe symptoms are associated with worse outcomes.2,11–16
However the mortality is 3-4% within three months of the onset of symptoms and thereafter 7% on a six month surgical waiting list. It is therefore vital to ensure that symptoms are reliably reported and an exercise test may be needed to check that a patient is genuinely asymptomatic. The duration of the asymptomatic phase varies widely between patients and the onset of symptoms is unpredictable. This is why regular follow-up of asymptomatic patients in a specialist valve clinic, combined with prompt surgical referral once symptoms develop, has been shown to result in outcomes similar to that of an age- and gender-matched population.17
The purpose of this module is to review some of the major pathophysiological mechanisms that underlie heart valve disease.1 Whilst these account for the vast majority of patients seen on a clinical basis, it should be remembered that there are numerous rarer causes of valve disease that are beyond the scope of this review. These include congenital defects and acquired conditions related to an array of systemic diseases, tumours, toxins and drugs.
Normal valvular structure
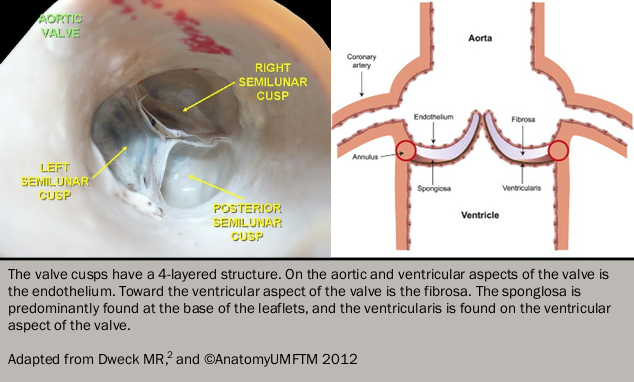
All four cardiac valves share similarities in their basic structure and histological appearances. Externally the leaflets are lined with endothelium and consist of two central layers: the fibrosa and spongiosa. The fibrosa provides strength and structural support for the valve, consisting predominantly of fibroblasts, collagen and elastin fibres. In contrast, the spongiosa is soft and compressible, consisting of mucopolysaccharides and mesenchymal cells, which absorb compressive forces within the valve and providing flexibility to allow the leaflets to change conformation as they open and close (see figure 12). The function of the atrioventricular (mitral and tricuspid) valves also depends on the actions of the chordae tendinae: tendon-like structures consisting of collagen and elastin fibres covered with endothelia which maintain valve competency during ventricular systole.
Figure 1. The normal structure of the trileaflet aortic valve
Calcific valve disease
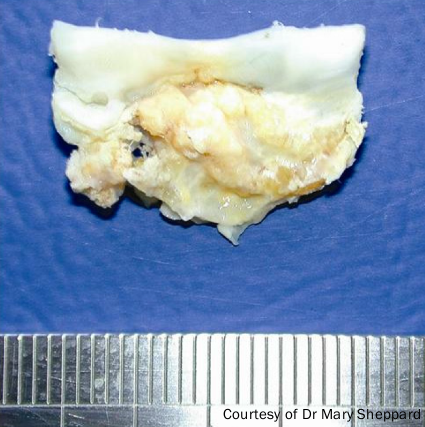
Figure 2. Example of calcification of aorta, a common cause of aortic stenosis
This is perhaps best exemplified by calcific aortic stenosis (see figure 2). Once believed to be the result of prolonged wear and tear and an inevitable consequence of ageing, this common condition is now recognised to be an active, highly-regulated inflammatory condition with common risk factors and similar pathological characteristics to atherosclerosis.3
Aortic stenosis
Progressive narrowing of the aortic valve results from increased thickening and stiffness of the valve leaflets, which restricts their opening and imposes an increased afterload on the left ventricle. Mechanical stress is believed to act as the initiating trigger. This causes damage to the endothelium on the aortic aspect of the valve, facilitating the infiltration of inflammatory cells and lipid. This is believed to be a two stage process, with an initiation phase resulting from endothelial injury and inflammatory cell infiltration and a propagation phase resulting in progressive calcification.4 The pathophysiology is shown in figure 3.4